Dysbiotic Gut Microbiota Depletes Amino Acids and Triggers Depression in Youth
Depression in children and adolescents affects 4–5% of youth worldwide, with rates climbing steeply over the past decade. Conventional treatment targets serotonin—but new evidence reveals that’s only half the story. A landmark multi-omics study discovered that depressed youth have depleted plasma amino acids paired with dysbiotic bacteria that cannot synthesize them, and that this amino acid deficiency directly contributes to mood disorder pathology. When bacteria from depressed children were transplanted into healthy adolescent rats, the animals developed depression-like behaviors along with the same amino acid depletion. The mechanism: lysine restriction alone was sufficient to trigger depressive behavior by suppressing glutamate transporters in the developing brain.
Key Findings
- Thirteen amino acids are significantly depleted in plasma of depressed youth (256 MDD patients vs. 307 healthy controls), with lysine showing the most dramatic reduction
- An amino acid signature predicted depression with 97.8% diagnostic accuracy (ROC-AUC = 0.978)—near-perfect discrimination between depressed and healthy adolescents
- 58 bacterial taxa are enriched and 46 are depleted in stool samples of depressed youth, with six distinct amino acid metabolism modules disrupted across the microbiota
- Procrustes analysis revealed strong association between altered gut microbiome composition and circulating amino acid metabolism (p-value = 0.001, M² = 0.932)
- Fecal microbiota transplant from depressed children to antibiotic-treated adolescent rats induced depression-like behaviors and replicated 14-amino acid deficiency in the prefrontal cortex
- Dietary lysine restriction alone triggered depression-like behavior in adolescent rats by reducing glutamate transporter expression in the prefrontal cortex
Source: Microbiome (2025) | Teng et al.
A 97.8% Accurate Amino Acid Signature for Pediatric Depression
The study enrolled 563 children and adolescents aged 10–18 (256 with major depressive disorder, mean age 15.4 years, 73.4% female; 307 healthy controls, mean age 15.3 years, 67.4% female). High-resolution plasma metabolomics identified 360 differentially expressed metabolites, with amino acid metabolism showing the most disrupted pathway (p < 0.0001). Thirteen of the 20 essential and semi-essential amino acids were significantly depleted—including eight that the body cannot synthesize (lysine, methionine, tryptophan, isoleucine, leucine, phenylalanine, valine, histidine) and five others critical for neuronal function (cysteine, tyrosine, arginine, glutamine, and elevated glutamic acid).
When machine learning models trained on these amino acid profiles alone to classify depressed versus healthy youth, they achieved a receiver operating characteristic area under the curve of 0.978—a level of accuracy rarely achieved in psychiatry. To contextualize: clinical biomarkers with AUC above 0.9 are considered exceptional. This finding raises an urgent question: should pediatricians implement plasma amino acid screening as a standard objective measure for depression diagnosis and risk stratification in adolescents?
Dysbiotic Shifts in Bacterial Families and Amino Acid Synthesis Pathways
Fecal metagenomic analysis from 83 depressed youth and 58 healthy controls revealed systematic bacterial dysbiosis. The researchers identified 58 bacterial taxa enriched in depression (p < 0.05, LDA > 2) and 46 taxa depleted—a far more pronounced shift than typically observed in adult depression. The inflammatory bacterium Eggerthellaceae was overabundant, while protective short-chain fatty acid producers (Faecalibacterium prausnitzii and Bifidobacterium animalis) were severely depleted. The pathogenic genus Akkermansia, linked to autoimmunity and neuroinflammation, was elevated.
Beyond taxa abundance, functional analysis revealed that six distinct bacterial metabolic modules for amino acid synthesis and degradation were significantly altered. Pathways for lysine, arginine, and tryptophan metabolism—all essential for serotonin and glutamate homeostasis—were disrupted. This dysbiotic microbiota had systematically lost the metabolic capacity to synthesize amino acids that the developing brain critically needs. Procrustes analysis confirmed strong coupling between bacterial composition changes and circulating amino acid depletion (p = 0.001, M² = 0.932), suggesting the dysbiotic state directly drives metabolic insufficiency.
Causal Proof: Fecal Transplant Replicates Amino Acid Deficiency and Depressive Behavior
To establish causation beyond correlation, the team performed fecal microbiota transplantation. Researchers transferred bacteria-free stool suspension from depressed children and adolescents into antibiotic-treated adolescent rats. The results were striking: rats receiving dysbiotic microbiota from depressed youth developed robust depressive-like behaviors on standard behavioral tests and exhibited the identical 14-amino acid deficiency in the prefrontal cortex that was observed in the original human patients. This causal transfer proves that the dysbiotic microbial community directly contributes to the neurochemical deficiency.
The team then tested lysine specifically. Adolescent rats exposed to chronic mild stress and fed a lysine-restricted diet showed significantly elevated depression-like behaviors compared to controls. Mechanistically, lysine restriction reduced expression of excitatory amino acid transporters (EAATs) in the prefrontal cortex—proteins that clear glutamate from synapses. Without adequate lysine, these critical transporters cannot function properly, glutamate accumulates, and the brain enters a state of excitotoxicity that drives mood dysregulation.
Why Lysine Deficiency Specifically Undermines Mood Regulation
Lysine is an essential amino acid—humans cannot synthesize it and must obtain it from food or microbial sources. Beyond serving as a protein building block, lysine is a precursor for carnitine, which fuels neuronal energy metabolism, and it is required for synthesis of proteins involved in neurotransmitter regulation. Most critically for mood, lysine supports expression and function of excitatory amino acid transporters that maintain glutamate homeostasis.
The prefrontal cortex is exquisitely sensitive to glutamate balance. Under healthy conditions, EAATs rapidly remove glutamate from synapses after neural firing, maintaining signaling fidelity. When lysine is depleted, EAAT expression drops, glutamate clearance fails, and the neuron experiences excitotoxic damage that disrupts the circuits maintaining mood stability. Additionally, tryptophan depletion—also observed in the study—reduces brain serotonin synthesis, creating a dual monoamine deficit. The study found that 5-hydroxytryptophan, an intermediate in serotonin synthesis, was dramatically downregulated in depressed youth.
Brain Connectivity Deficits Correlated with Amino Acid Dysregulation
Resting-state functional MRI from 111 depressed youth and 51 healthy controls revealed disrupted functional connectivity between the prefrontal cortex and temporal and subcortical regions. These connectivity deficits were not random—they correlated significantly with both depressive symptom severity (HAMD-24, p < 0.001) and the degree of amino acid dysregulation (22 specific DEMs in amino acid metabolism, p < 0.05). This suggests that amino acid depletion does not simply affect mood through single-cell mechanisms but actively reshapes the large-scale neural networks that support emotional regulation, executive control, and reward processing during a critical developmental window.
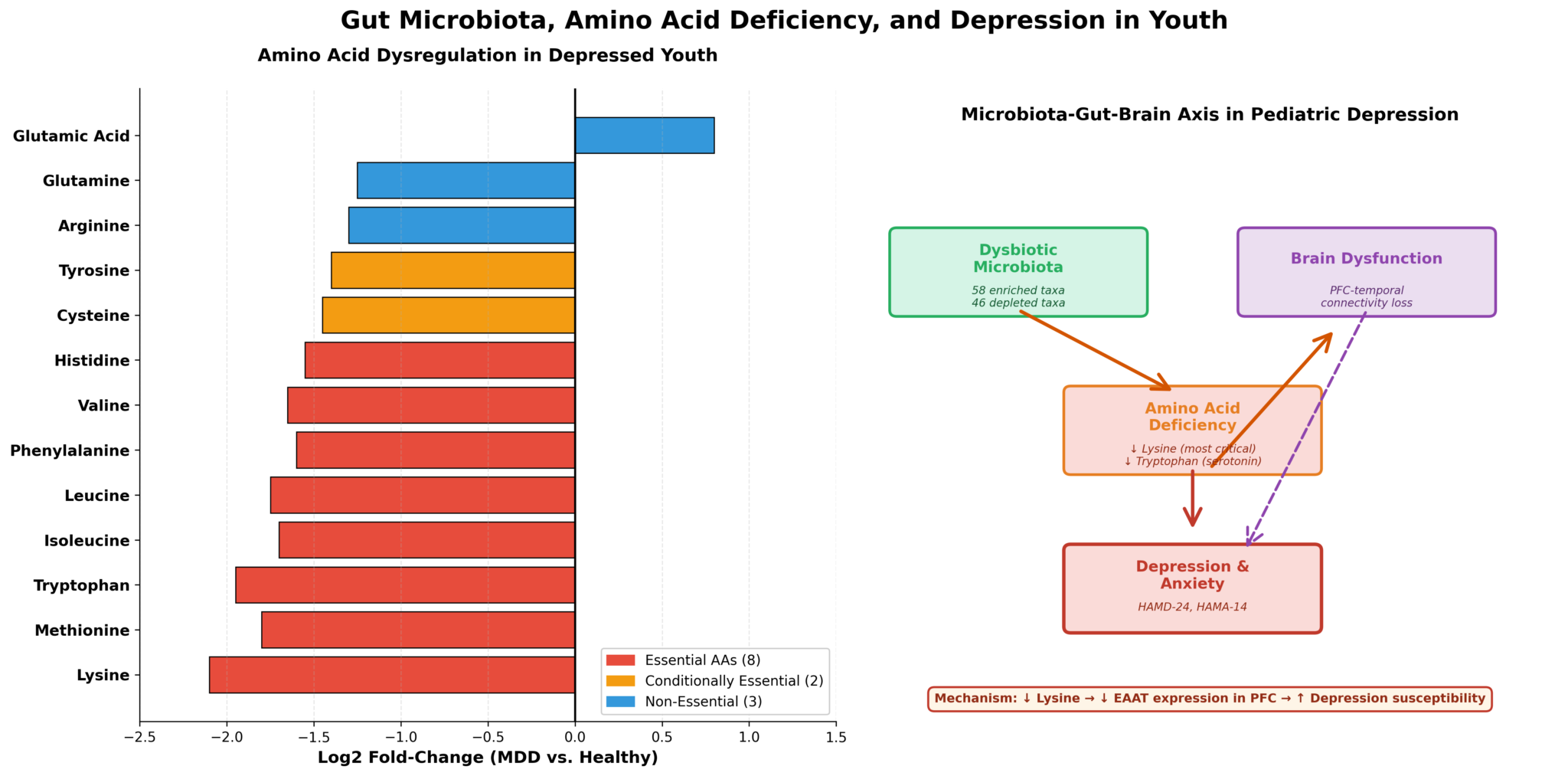
Image file: gut-microbiota-amino-acids.png — Plasma amino acid dysregulation in depressed youth (N = 256 MDD vs. 307 controls); lysine shows the most dramatic reduction
Targeting the Microbiota-Amino Acid Axis as a Novel Treatment Strategy
Objective amino acid screening as a depression biomarker: The 97.8% diagnostic accuracy of amino acid profiles suggests that plasma amino acid testing could become a standard diagnostic tool. Rather than relying solely on symptom questionnaires, pediatricians could integrate amino acid profiling as an objective measure of depression risk. This is particularly valuable for adolescents who minimize or deny mood symptoms.
Dietary and microbiota-targeted interventions: The causal role of dysbiosis and amino acid depletion opens therapeutic pathways. Dietary strategies include increasing lysine (poultry, eggs, legumes, pumpkin seeds), tryptophan (turkey, cheese, nuts, seeds), and methionine (fish, meat, dairy); targeted probiotics or prebiotics designed to restore amino acid-synthesizing bacterial species; and dietary patterns that favor short-chain fatty acid-producing bacteria (high fiber, diverse plant foods). For adolescents with treatment-resistant depression, microbiota-targeted interventions could serve as a first-line adjunct to conventional antidepressants.
Precision psychiatry during development: Adolescents have substantially higher metabolic demands for amino acids due to rapid physical growth and ongoing prefrontal cortex maturation. If the dysbiotic microbiota cannot meet these elevated demands during this critical window, the consequences for mood regulation, executive function, and long-term brain health are severe. This developmental sensitivity may explain why standard antidepressants have modest efficacy in youth and why prevention through dietary optimization and microbiota health could be especially powerful during adolescence.
Future microbiome-based diagnostics and therapeutics: This work establishes a template for precision microbiome medicine. Refinement could yield predictive models integrating specific bacterial taxa and metabolite signatures for personalized depression risk; identification of therapeutic bacterial strains or bacteriophages; and engineered probiotic therapies designed to restore amino acid biosynthesis. Such targeted approaches could transform pediatric depression diagnosis and treatment.
Citation: Teng, T., Huang, F., Xu, M., Li, X., Zhang, L., Yin, B., Cai, Y., Chen, F., Zhang, L., Zhang, J., Geng, A., Chen, C., Yu, X., Sui, J., Zhu, Z.-J., Guo, K., Zhang, C., & Zhou, X. (2025). Microbiota alterations leading to amino acid deficiency contribute to depression in children and adolescents. Microbiome, 13, 128. doi:10.1186/s40168-025-02122-w
Authors’ affiliations: Department of Psychiatry, Chongqing Medical University; Center for Brain Disorders and Cognitive Science, Chongqing Medical University; Institute of Biomedical Sciences, Fudan University, Shanghai, China.