TL;DR: A 2026 medRxiv preprint found that one session of repetitive transcranial magnetic stimulation (rTMS) over the left dorsolateral prefrontal cortex (DLPFC) reduced cigarette craving in adults with tobacco use disorder, and the people who responded had heavier baseline smoking, craving, and withdrawal.
Key Findings
- DLPFC craving test: The randomized crossover study included 60 adults with tobacco use disorder who smoked at least 5 cigarettes per day for at least 1 year.
- DLPFC beat V5: rTMS over the left DLPFC reduced Shiffman-Jarvik Withdrawal Scale craving scores (t(59)=3.6410, p=0.0006), while stimulation of visual cortex V5 did not reach significance.
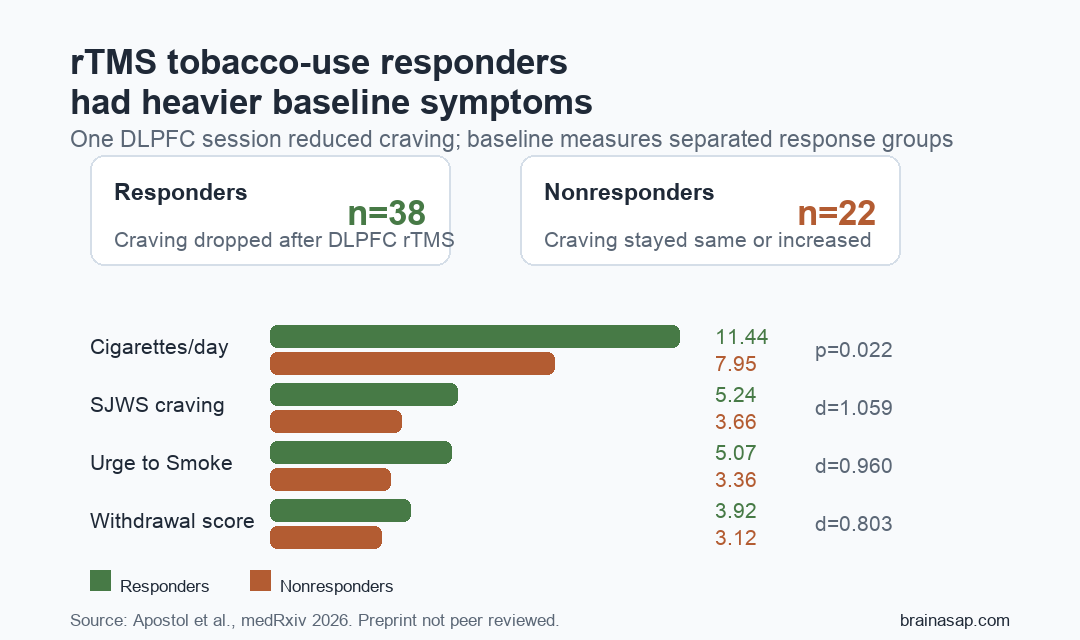
- 38 responders identified: Researchers classified 38 participants as responders after any craving reduction and 22 as nonresponders after no change or worsening.
- Baseline smoking differed: Responders smoked more cigarettes per day before treatment than nonresponders (11.44 vs 7.95; p=0.022).
- Exploratory connectivity differed: Responders had reduced insula-to-right-nucleus-accumbens connectivity compared with nonresponders (left insula d=-0.924; right insula d=-0.822).
Source: medRxiv (2026) | Apostol et al.
Repetitive transcranial magnetic stimulation (rTMS) is already used in psychiatry, but tobacco use disorder creates a harder prediction problem: not every smoker has the same craving biology, and a time-intensive brain-stimulation treatment needs better responder markers.
This preprint tested a short-term version of that question. Researchers asked whether craving response after one rTMS session could be separated by baseline smoking severity, withdrawal symptoms, and functional MRI connectivity patterns.
One DLPFC rTMS Session Reduced Cigarette Craving
The study used a within-subjects randomized crossover design. Each participant received active rTMS over the left DLPFC and active control stimulation over visual cortex V5, with the order randomized and the sessions separated by at least 24 hours.
Participants were adults with tobacco use disorder who smoked at least 5 cigarettes per day for at least 1 year. They were asked to abstain from tobacco for at least 12 hours before each rTMS appointment, with abstinence checked by expired carbon monoxide and self-reported last cigarette time.
- Experimental target: Left DLPFC, a prefrontal region involved in executive control and top-down regulation.
- Control target: Left V5, a visual cortex region used as an active control site rather than sham stimulation.
- Stimulation dose: 10 Hz rTMS, 60 trains, and 3000 pulses total at 100% active motor threshold.
- Main acute outcome: Change in the Shiffman-Jarvik Withdrawal Scale craving subscale before versus after stimulation.
DLPFC stimulation significantly reduced craving scores (t(59)=3.6410, p=0.0006). V5 stimulation did not produce a statistically significant craving reduction (p=0.0718).
Responders Smoked More and Reported More Withdrawal
Researchers defined 38 responders as participants whose craving score decreased after DLPFC rTMS. The remaining 22 nonresponders had no improvement or a higher craving score.
Baseline smoking behavior separated the groups. Responders reported 11.44 cigarettes per day in the prior 30 days, compared with 7.95 cigarettes per day among nonresponders (p=0.022).
Several symptom measures also showed large responder/nonresponder differences immediately before DLPFC rTMS:
- SJWS craving: Responders averaged 5.242 versus 3.664 in nonresponders, with Cohen’s d=1.059.
- Overall withdrawal: Responders averaged 3.919 versus 3.121, with Cohen’s d=0.803.
- Urge to Smoke: Responders averaged 5.066 versus 3.359, with Cohen’s d=0.960.
Pre-Registered Connectivity Tests Were Mostly Negative
The neuroimaging results were not a simple biomarker win. Pre-registered functional connectivity tests focused on DLPFC-to-orbitomedial-prefrontal cortex, DLPFC-to-inferior-parietal lobule, and insula seed-based connectivity.
Those planned connectivity comparisons did not significantly separate responders from nonresponders after correction. DLPFC-OMPFC connectivity, DLPFC-IPL connectivity, and the whole-insula seed analyses were all negative under the original responder definition.
- DLPFC-OMPFC: Pre-rTMS connectivity did not differ significantly between groups (p=0.199).
- DLPFC-IPL: Pre-rTMS connectivity did not differ significantly between groups (p=0.361).
- Connectivity change: DLPFC-OMPFC and DLPFC-IPL change scores also did not differ between responders and nonresponders.
- Insula seeds: Whole-insula and insula-subregion analyses did not survive correction under the pre-registered approach.
The negative planned analyses narrow which candidate rTMS-response markers survived the pre-registered test and which findings should be treated as exploratory.
Exploratory Insula-Reward Connectivity Separated Stronger Responders
Exploratory analyses used a stricter response definition: the roughly top third of participants with at least a 1-point craving reduction. Under that definition, nonresponders had stronger insula connectivity with occipital and parietal regions, including the occipital pole and precuneus.
Region-of-interest analyses also found that responders had reduced functional connectivity between the insula and right nucleus accumbens, a reward-related region. The left insula-to-right-nucleus-accumbens difference had corrected p=0.005 and Cohen’s d=-0.924; the right insula-to-right-nucleus-accumbens difference had corrected p=0.016 and Cohen’s d=-0.822.
Those connectivity findings are not the same as confirmed clinical selection rules. They suggest that an abstinence-state salience/reward network may differ in people whose craving is more modifiable after DLPFC stimulation.
Single-Session Design Limits Smoking-Cessation Claims
The study measured acute craving change after one rTMS session, not durable abstinence after a full treatment course. Multi-session protocols are usually needed for clinically meaningful smoking-cessation outcomes.
Several limits keep the clinical interpretation narrow:
- Small sample: The final analysis included 60 participants, and 3 participants were excluded from neuroimaging analyses because of incomplete functional MRI scans.
- Acute endpoint: Craving reduction after one appointment is not the same as quitting smoking.
- Self-report outcomes: Craving and withdrawal scales were the main response measures, even though abstinence was biochemically checked.
- Exploratory imaging: The most specific insula-NAc findings were not part of the original pre-registered analysis plan.
The most defensible use is responder-marker development for future rTMS trials in tobacco use disorder. Baseline craving, withdrawal, cigarette consumption, and insula-reward connectivity are candidates to test prospectively, not proof that a single rTMS session can produce lasting cessation.
Citation: DOI: 10.64898/2026.06.23.26356059. Apostol et al. Determinants of Repetitive Transcranial Magnetic Stimulation Efficacy in Tobacco Use Disorder: A Pre-Registered Study. medRxiv. 2026.
Study Design: Pre-registered, single-blind, active-controlled randomized crossover rTMS experiment in adults with tobacco use disorder.
Sample Size: 60 adults in the final analysis; 38 responders and 22 nonresponders after DLPFC rTMS.
Key Statistic: DLPFC rTMS reduced craving scores (t(59)=3.6410, p=0.0006), and responders smoked more cigarettes per day before treatment than nonresponders (11.44 vs 7.95; p=0.022).
Caveat: The study tested acute craving after one rTMS session, and the strongest connectivity findings were exploratory rather than pre-registered confirmation.