TL;DR: A 2026 narrative review in Molecular Psychiatry argues that depression in Alzheimer’s disease and Parkinson’s disease follows disease-specific brain mechanisms, while standard antidepressant evidence remains weak in these neurodegenerative populations.
Key Findings
- 42% in Alzheimer’s disease: The review cites depressive syndromes affecting about 42% of patients with Alzheimer’s disease and 35% of patients with Parkinson’s disease.
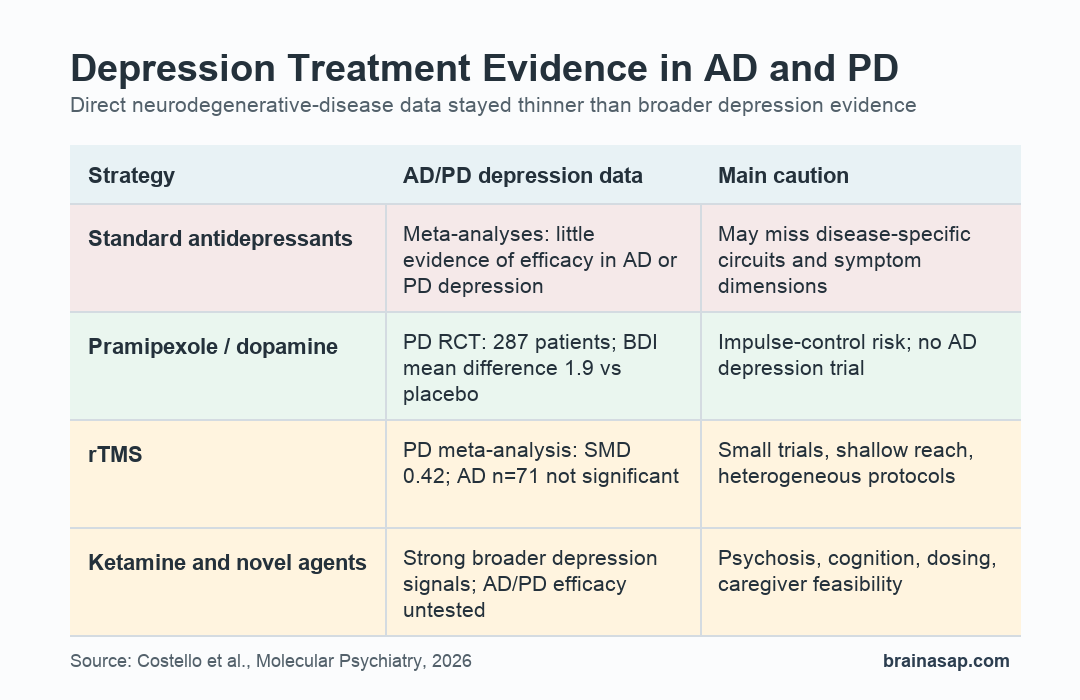
- Standard antidepressants underperformed: Meta-analyses found little evidence that existing antidepressants work well for depression in Alzheimer’s disease or Parkinson’s disease.
- Trial gap stayed large: Patients with cognitive impairment are often excluded from antidepressant trials, and few high-quality studies test new treatments directly in neurodegenerative disease.
- Pramipexole had direct PD data: In one Parkinson’s disease depression RCT with 287 patients, pramipexole improved Beck Depression Inventory scores by a mean difference of 1.9 points versus placebo.
- Brain-stimulation evidence was mixed: A Parkinson’s disease repetitive transcranial magnetic stimulation (rTMS) meta-analysis found modest benefit (SMD 0.42), while two small Alzheimer’s disease studies with 71 combined patients did not show a significant mood effect.
Source: Molecular Psychiatry (2026) | Costello et al.
Depression in neurodegenerative disease is not just depression that happens to occur in an older patient. The review focuses on Alzheimer’s disease (AD) and Parkinson’s disease (PD), where mood symptoms can track brain pathology, reward-circuit disruption, inflammation, medication state, and cognitive decline.
The practical problem is direct: people with AD or PD have high depression burden, but the treatment evidence has not kept up. The review’s central argument is that trials should stop assuming ordinary late-life depression biology will automatically apply to patients with neurodegeneration.
Depression Affected 42% of Alzheimer’s Patients and 35% of Parkinson’s Patients
The review cites depression rates of about 42% in Alzheimer’s disease and 35% in Parkinson’s disease. Those symptoms are associated with faster cognitive decline, poorer quality of life, higher mortality, and greater health-care use.
In Alzheimer’s disease, depression can appear as a risk factor, prodromal feature, or complication of established dementia. In Parkinson’s disease, depressive symptoms often overlap with apathy, anhedonia, medication-state changes, and frontostriatal reward-circuit dysfunction.
- Alzheimer’s disease: Mood symptoms can interact with amyloid, tau, serotonergic degeneration, cortical network disruption, and central neuroinflammation.
- Parkinson’s disease: Depression often sits closer to dopamine loss, reward learning, effort allocation, and motivational symptoms that worsen in the dopaminergic off state.
- Shared clinical burden: Both diseases create diagnostic overlap between depression, apathy, cognitive impairment, sleep disruption, and medication effects.
A global depression score can blur different symptom drivers. A patient whose main problem is low mood does not necessarily need the same intervention as a patient whose main problem is reward insensitivity, effort avoidance, or apathy.
Existing Antidepressants Showed Little Efficacy in AD and PD Depression
The review reports that meta-analyses show little or no efficacy for existing antidepressants in AD or PD depression. Individual patients still can respond, but the population-level evidence weakens the assumption that standard serotonin-focused prescribing solves the problem.
One reason is target mismatch. Neurodegenerative disease can damage the same systems that antidepressants depend on, including serotonergic projections, dopamine circuits, glutamatergic signaling, immune pathways, and cortical-subcortical networks.
- Neurotransmitter loss: AD and PD can alter serotonin, dopamine, glutamate, and receptor availability in disease-specific ways.
- Circuit-level symptoms: Anhedonia and apathy can reflect reward-circuit dysfunction more than a conventional mood syndrome.
- Trial exclusion: Cognitive impairment often keeps patients out of antidepressant trials, leaving clinicians to extrapolate from younger or less neurologically complex groups.
Vortioxetine illustrates the problem. The drug has serotonergic and cognitive-interest logic, but a randomized trial with 100 patients with AD depression failed to show benefit versus placebo.
The review therefore treats depression in AD and PD as a treatment-development problem, not only a prescribing problem. Better trials need to match the intervention to the biology and symptom profile being tested.
Glutamate and Dopamine Targets Look Plausible but Unevenly Tested
Ketamine has strong evidence for rapid antidepressant effects in treatment-resistant depression outside neurodegenerative disease. The review notes a meta-analysis of seven ketamine trials with 373 participants, showing a 24-hour depressive-symptom reduction with SMD -0.77.
That evidence does not directly answer AD or PD depression. Ketamine has not been tested for efficacy in those populations, and older adults with dementia or PD face higher concern for dissociation, psychosis, blood-pressure effects, and treatment logistics.
The most directly relevant dopamine signal was pramipexole, a D2/3 dopamine-receptor agonist. In a Parkinson’s disease depression RCT with 287 patients, pramipexole improved depressive symptoms at 12 weeks, independent of motor improvement.
- Pramipexole advantage: The mechanism fits PD motivational symptoms because D3 receptors are concentrated in mesolimbic reward circuits.
- Pramipexole risk: Dopamine agonists can increase impulse-control disorders, including gambling, hypersexuality, and compulsive shopping.
- AD uncertainty: Dopamine changes occur in some Alzheimer’s disease cases, but pramipexole has not been evaluated for AD depression.
The review also discusses dextromethorphan-bupropion, prucalopride, psychedelics, pimavanserin, KCNQ channel modulators, and kappa opioid receptor therapies. Most remain biologically plausible rather than clinically established for neurodegenerative depression.
Neuromodulation May Fit Circuit Symptoms Better Than Standard Drug Trials
Repetitive transcranial magnetic stimulation (rTMS) already has established depression efficacy in general psychiatric use. In neurodegenerative disease, the review found a more limited pattern: modest benefit in PD, unclear benefit in AD.
A meta-analysis of seven double-blind PD trials found rTMS benefit versus sham, with SMD 0.42. The largest included RCT had only 44 participants, and protocols differed across studies.
For Alzheimer’s disease, two small studies with 71 combined patients did not show a significant effect on depressive symptoms. That may reflect weak efficacy, insufficient sample size, poor target matching, or difficulty measuring depression cleanly in dementia.
- rTMS limitation: Standard stimulation is shallow, roughly 2 cm, which limits access to deeper reward and motivation circuits.
- tDCS possibility: Home-based transcranial direct current stimulation is scalable in principle, but it has not been tested specifically for depression in AD or PD.
- Focused ultrasound: Low-intensity ultrasound could target deeper reward circuits, but depression evidence is still early-phase.
- DBS context: Deep brain stimulation is most relevant for severe PD cases already receiving DBS, but dedicated PD depression trials are lacking.
The strongest neuromodulation message is not that one device is ready for broad use in AD or PD depression. It is that circuit-level symptoms need circuit-level treatment designs.
Future Trials Need Biomarkers, Symptom Dimensions, and Safety Filters
The review calls for biomarker-informed trials rather than broad depression studies that enroll heterogeneous older adults. A dopamine-targeted trial, for example, should prioritize patients with reward-processing impairment, prominent motivational symptoms, or evidence of striatal dysfunction.
Inflammation studies need similar stratification. About one-third of depression patients show elevated C-reactive protein above 3 mg/L in broader depression research, but anti-inflammatory trials in unselected samples have often been modest or negative.
For Alzheimer’s disease, central microglial activation and cortical network dysfunction matter more than peripheral inflammation alone. For Parkinson’s disease, peripheral inflammatory changes appear less directly tied to depressive symptoms, which changes the treatment logic.
- Match mechanism to symptom: Reward-circuit therapies should test anhedonia, apathy, and effort-based decision-making, not only total depression scores.
- Build in biomarkers: Trials could use p-tau217, monoaminergic positron emission tomography (PET) imaging, inflammatory markers, functional connectivity, or disease-stage measures.
- Filter for tolerability: Ketamine, psychedelics, dopamine agonists, and invasive stimulation require extra caution in patients vulnerable to psychosis, confusion, falls, polypharmacy, or caregiver burden.
The review’s clinical implication is cautious but useful. Depression in AD and PD can become a better test case for precision psychiatry because the disease process can be mapped across biomarkers, circuits, behavior, and time.
For now, the paper supports better trial design more strongly than it supports any new routine treatment. The next step is to test plausible interventions in the actual neurodegenerative populations that standard antidepressant studies have often left out.
Citation: DOI: 10.1038/s41380-026-03728-8. Costello et al. Depression in neurodegenerative disease: neurobiological mechanisms and emerging treatments. Molecular Psychiatry. 2026.
Study Design: Narrative review of mechanisms and emerging treatments for depression in Alzheimer’s disease and Parkinson’s disease.
Sample Size: Source synthesis includes molecular imaging, neuropathology, cognitive neuroscience, and clinical-trial evidence rather than one pooled patient sample.
Key Statistic: Depression affects about 42% of patients with Alzheimer’s disease and 35% of patients with Parkinson’s disease, while standard antidepressant evidence remains weak in these groups.
Caveat: Many treatment signals come from non-neurodegenerative depression studies or small disease-specific trials, so routine clinical claims require larger AD and PD trials.