TL;DR: Aerobic exercise matches antidepressant efficacy for depression with effect size −1.60, resistance training slightly edges aerobic for anxiety, and neither requires meeting WHO guidelines—20 minutes three times weekly still produces clinical improvement.
Depression responds to a treatment that’s free, legal, and accessible: exercise. But the type matters profoundly.
A comprehensive meta-analysis of 26 randomized controlled trials involving 2,681 adults with clinical depression or anxiety reveals an unexpected divergence: aerobic training dominates depression, while resistance training edges ahead for anxiety.
Most startling: you don’t even need to meet official exercise guidelines for symptoms to improve. Twenty minutes three times weekly produces real clinical improvement.
Key Findings
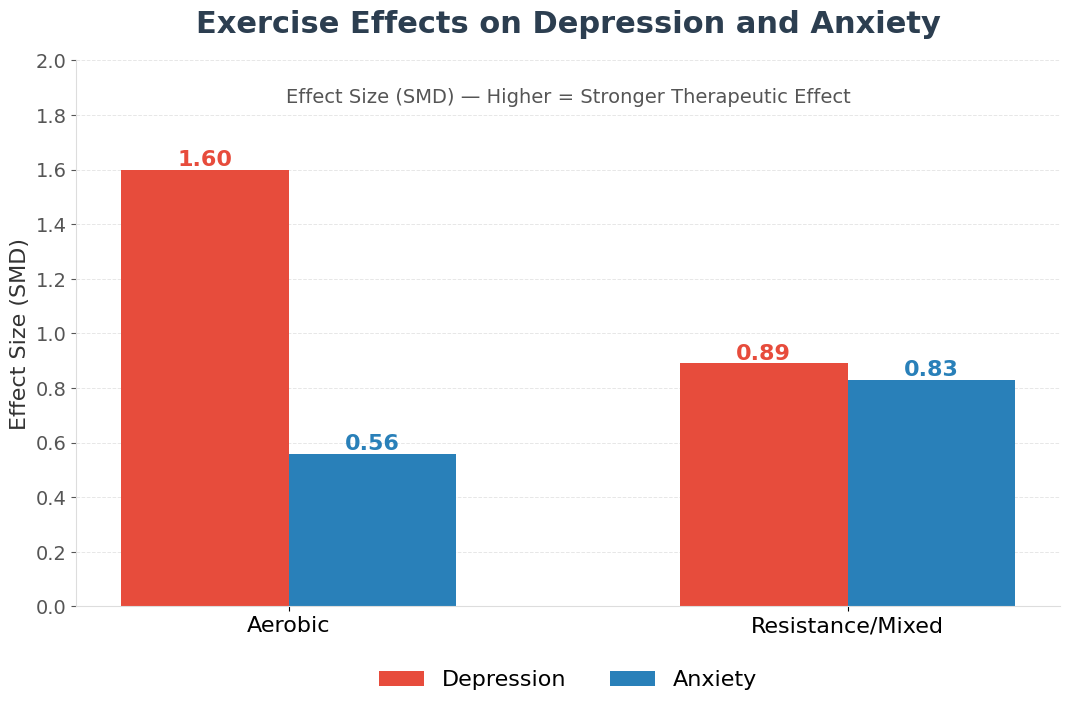
- Aerobic demolishes depression with effect size −1.60: Eighteen randomized trials of aerobic exercise produced standardized mean differences of −1.60, equivalent to antidepressant efficacy, substantially larger than resistance training’s −0.89 for the same condition.
- Resistance edges ahead for anxiety (slightly): Resistance training produced effect size −0.83 for anxiety versus aerobic’s −0.56—a numerical advantage that didn’t quite reach statistical significance (p = 0.683), suggesting evidence remains provisional.
- Sub-guideline exercise still triggers remission: Only 3 of 30 studies met WHO guidelines of 150 minutes weekly aerobic plus two resistance days. Yet all 30 produced clinically meaningful improvement. Twenty minutes, three times weekly works.
- Pharmaceutical-grade evidence: Sixty-seven percent of trials met CONSORT standards (the reporting benchmark for medication trials). This meta-analysis is as rigorous as antidepressant efficacy data—arguably more rigorous than typical psychiatric research.
- 2,681 adults across 17 countries and 5 continents: Trials ranged from 2 weeks to 12 months duration. These were clinically diagnosed populations, not subclinical mild-mood fluctuations.
- Substantial variation in exercise response: High heterogeneity (I² = 90.1% for depression) reflects real-world differences in exercise intensity, duration, and population characteristics, but effect sizes remained robustly positive across all subgroups.
Source: International Journal of Mental Health Nursing (2025) | Banyard et al.
Why Aerobic Exercise Demolishes Depression Like Medication Does
Eighteen randomized trials found that aerobic exercise produces an effect size of −1.60 for depression—matching antidepressant medication. A person with clinical depression who walks, jogs, or cycles at moderate intensity for 30 minutes three times weekly improves as much as someone on an SSRI.
Resistance training also helps depression, but the effect size (−0.89) is notably smaller. Why does aerobic exercise dominate depression? Several mechanisms converge:
- Stress hormones reset: Aerobic exercise resets the dysregulated HPA axis, lowering cortisol and restoring its normal circadian rhythm.
- Neurotransmitter boost: Aerobic activity increases serotonin and dopamine availability—the exact neurotransmitters that antidepressants modulate.
- Neurogenesis: Aerobic exercise elevates BDNF (brain-derived neurotrophic factor), the signal that promotes new neuron growth in the hippocampus, a region shrunken in depression.
- Anti-inflammation: Aerobic exercise is one of the most potent anti-inflammatory interventions known, reducing cytokines that depression elevates.
Resistance training offers some of these benefits, but aerobic activity appears more efficient for mood regulation.
Practically: if you’re depressed, aerobic exercise should be your first recommendation. You don’t need marathons—a 30-minute walk three times weekly at conversational pace produces real symptom improvement.
You don’t need to meet guideline volumes. You don’t need a gym. You need consistency and moderate intensity. That’s it.
Resistance Training’s Slight Edge Against Anxiety (With an Important Caveat)
Anxiety told a different story. Aerobic exercise for anxiety produced effect size −0.56—modest, clinically meaningful but not impressive. Resistance training or mixed modalities produced −0.83—noticeably larger.
But here’s the caveat: the difference didn’t reach statistical significance (p = 0.683). With anxiety evidence based on only 12 trials versus 26 for depression, the apparent advantage could reflect random noise in smaller sample sizes rather than true superiority. Be cautious before celebrating resistance training as clearly better for anxiety, but the trend is worth attention.
If resistance training does hold an edge for anxiety, the mechanism likely involves mastery and progressive challenge. Anxiety hinges on learned helplessness—the belief that threats are uncontrollable. Resistance training, with its progressive overload (lifting heavier each week) and quantifiable strength gains, directly targets this problem.
You see yourself getting stronger. That tangible evidence of control may combat anxiety’s core “I’m helpless” distortion more effectively than aerobic activity.
The practical recommendation: if you’re anxious, try resistance training first. But if you hate weights and love running, run. The evidence gap is small enough that preference and adherence probably outweigh modality effects.
The Discovery That Changes Everything: You Don’t Need to Meet Guidelines
Here’s the finding that should reshape how clinicians and patients approach exercise for mental health. Only 3 of 30 studies met WHO guidelines—150 minutes weekly of aerobic plus two resistance days. Yet all 30 studies produced clinically meaningful improvement.
Most prescribed far less: 20 to 40 minutes, two to four times weekly. Sub-guideline exercise produced real symptom reduction.
This demolishes a pervasive myth: patients believe exercise only “counts” at prescribed volumes. But the evidence says a 20-minute walk three times weekly is a win. Don’t abandon it for a perfect routine you won’t maintain.
Start absurdly small—15 minutes twice weekly—and build from there. The psychological victory of “I exercised and felt better today” drives adherence. Consistency at low volume beats ambitious plans abandoned in frustration.
Why This Evidence Rivals Antidepressant Efficacy Studies
The quality of evidence deserves emphasis. Sixty-seven percent of trials met CONSORT reporting standards—the gold-standard checklist used for medication trials. This is pharmaceutical-grade evidence that exercise works for depression and anxiety.
Caveats and limitations:
- Missing methodological details: Only 28% of trials reported power calculations. Many omitted exercise prescription details—supervised or home-based? What intensity? These gaps make identifying the optimal “dose” harder.
- Small sample bias: Seven trials enrolled 30 or fewer participants. Small studies tend to report inflated effect sizes, so true effects are likely somewhat more modest than reported, especially for anxiety.
- Conservative interpretation still positive: Even accounting for these inflations, the effects remain clinically meaningful. Benefits were strongest in people with clinically diagnosed depression or anxiety, not mild mood fluctuations.
In practice, this means: if you have clinical depression—the kind that disrupts sleep, appetite, and function—exercise’s effects are dramatic. If you’re mildly sad sometimes, exercise helps. The magnitude of benefit scales with severity of the underlying condition.
If You’re Depressed: Aerobic Exercise as First-Line Treatment
Clinical evidence now supports aerobic exercise as a first-line treatment for mild to moderate depression. Walking, jogging, cycling, or swimming at moderate intensity for 30 minutes three times weekly produces symptom improvements matching antidepressant medication.
You don’t need to hit WHO targets of 150 minutes weekly. You don’t need the gym. You need consistency.
For severe depression—especially when suicide risk, hospitalization, or complete functional collapse is present—exercise complements but doesn’t replace medication and psychotherapy. It’s adjunctive, not monotherapy. But for mild to moderate depression, the evidence is clear: start aerobic exercise.
If You’re Anxious: Resistance Training with a Caveat
Resistance training shows a slight numerical advantage for anxiety (effect size −0.83 versus −0.56 for aerobic), though the evidence base is smaller and the difference doesn’t reach statistical significance. If you’re anxious, try resistance training first.
But if you hate the gym and love running, run—the evidence gap is small enough that your preference matters. Plan for 20–40 minutes, two to four times weekly. Don’t aim for guideline volumes; aim for consistency you’ll maintain.
How to Actually Start (And Stick With It)
- Be specific about time and place. Not “I’ll exercise more” but “Monday, Wednesday, Friday at 6 PM, a 20-minute walk from my house.” Specificity predicts adherence better than good intentions.
- Abandon perfect for sustainable. Sub-guideline exercise (20–40 minutes, two to four times weekly) produces real benefit. A realistic plan beats a heroic one that fails by week two.
- Pick the type you’ll genuinely do. Aerobic owns depression, resistance holds a slight edge for anxiety. But the best exercise is the one you’ll actually do. Movement matters more than modality.
- Mix if boredom threatens. Many trials used mixed protocols: some days aerobic, some days resistance. This reduces monotony and lets you vary your exercise mindset.
- Combine with medications if needed. Exercise and antidepressants synergize. Adding exercise to medication produces better outcomes than either alone.
- Celebrate small wins. You need the victory of “I exercised and felt better today.” That feedback loop is what sustains long-term adherence.
The Evidence That Exercise Is Medicine
Depression crumbles under aerobic exercise producing an effect size of −1.60 for depression, matching antidepressant medication. Anxiety shrinks with resistance training’s slight edge, though smaller evidence bases make this tentative. The transformative finding: you don’t need perfect exercise.
Sub-guideline work—20 to 40 minutes, two to four times weekly—produces real symptom reduction. This meta-analysis, with 67% of trials meeting pharmaceutical reporting standards, justifies treating exercise as first-line treatment for mild to moderate depression.
For people avoiding medications or preferring non-pharmacological approaches, the path is clear: aerobic work for depression, resistance for anxiety. Don’t force yourself into an exercise type you hate. Start today with what you’ll sustain. The science says you will feel better.
Full Citation: Banyard H, Edward KL, Garvey L, Stephenson J, Azevedo LA, Benson AC. The effects of aerobic and resistance exercise on depression and anxiety: A systematic review and meta-analysis of randomised controlled trials. International Journal of Mental Health Nursing. 2025;34(2):e70054. DOI: 10.1111/inm.13480
Study Design: Systematic review and meta-analysis of 26 randomized controlled trials across 17 countries with 2,681 adults with clinically diagnosed depression or anxiety
Key Effect Sizes: Aerobic for depression: SMD = −1.60; Resistance for depression: SMD = −0.89; Aerobic for anxiety: SMD = −0.56; Resistance for anxiety: SMD = −0.83
Study Quality: 67% met CONSORT reporting standards; heterogeneity I² = 90.1% for depression, 85.8% for anxiety
Lead Authors: Swinburne University of Technology, Victoria University, Federation University Australia, University of Huddersfield, Sheffield Hallam University