TL;DR: A 2026 systematic review in The British Journal of Psychiatry linked schizophrenia to a multisystem advanced-aging phenotype, including older-appearing brain scans, shorter telomeres, inflammation, and higher dementia risk.
Key Findings
- 170 studies included: The review synthesized studies of aging markers in schizophrenia and non-affective psychosis published after 2009.
- Most studies were moderate or high quality: 93 of 170 were rated high quality and 75 were rated moderate quality.
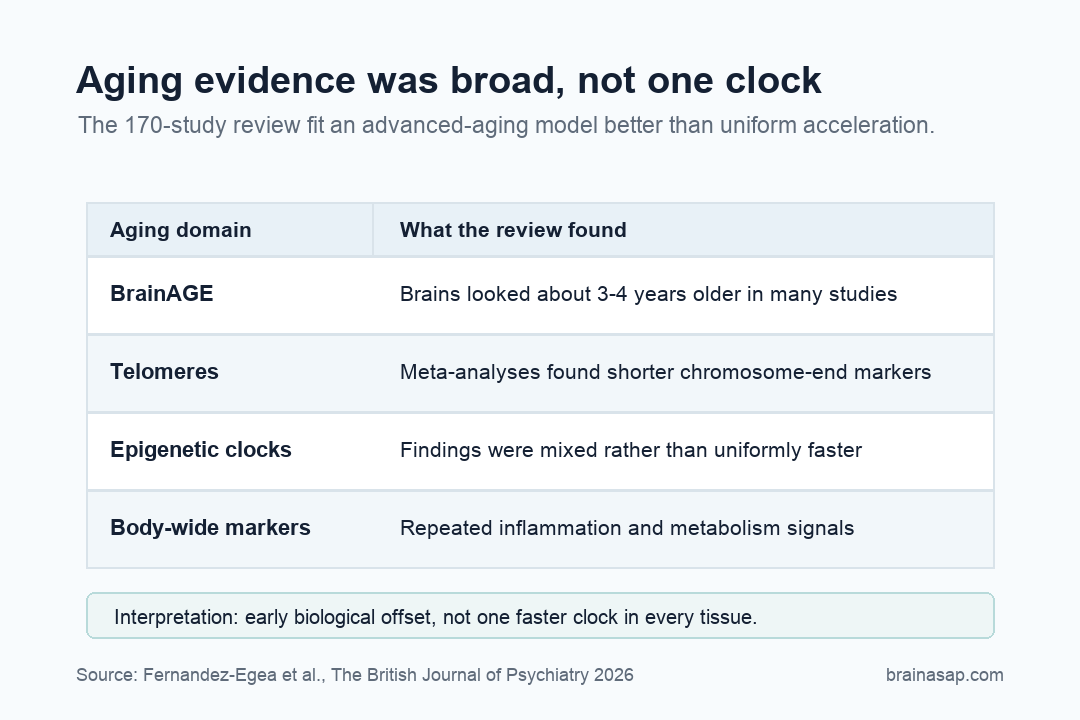
- Brain-age differences appeared early: BrainAGE studies showed mean differences of about 3 to 4 years, often present at first episode.
- Telomeres were consistently shorter: Meta-analyses reported standardized mean differences around -0.4 to -0.5.
- The evidence did not show simple acceleration: The review favored advanced aging: early biological deviation followed by more parallel decline.
Source: The British Journal of Psychiatry (2026) | Fernandez-Egea et al.
Schizophrenia is usually discussed as a psychiatric illness, but the body shows a broader illness profile. People with schizophrenia face earlier mortality, higher cardiometabolic burden, cognitive impairment, and increased dementia risk.
The review asked whether those outcomes are downstream complications or signs of altered biological aging.
The Review Tracked Aging Across Brain, Blood, and Metabolism
The accelerated-aging hypothesis was proposed in 2008 to explain why schizophrenia seemed linked to age-associated problems earlier in life.
Since then, researchers have tested the idea across mortality, dementia, cognition, brain imaging, telomeres, epigenetic clocks, inflammation, oxidative stress, and metabolism.
This review pulled those domains together. It followed PRISMA guidelines, was registered with PROSPERO, and focused on peer-reviewed studies after 2009, including meta-analyses and minimally treated or first-episode cohorts where possible.
Researchers identified 923 manuscripts and included 170 studies in the final synthesis. Quality was not uniformly weak: 93 studies were rated high quality and 75 moderate quality, with only 2 rated below that threshold.
That gives the review more weight than a loose narrative essay. The scope also matters.
Aging is not one measurement. It can mean several different measurement domains:
A convincing argument has to survive across several of those systems.
BrainAGE Gaps Pointed to an Early Biological Offset
The review makes a careful distinction. Uniform accelerated aging would mean the biological clock is running faster across systems.
Advanced aging means people start from an older biological position early, then may decline in parallel with peers.
The evidence leaned toward the second model. BrainAGE studies showed schizophrenia-associated brain-predicted age differences of roughly 3 to 4 years, often already visible around first episode.
Longitudinal evidence did not consistently show a steeper aging slope everywhere.
That distinction prevents a common overstatement. If a 25-year-old patient shows a brain-age estimate closer to 29, that does not automatically mean the brain will keep aging 4 years faster every decade.
It may mean the system diverged early and then continued along a different track.
The review also found converging clinical evidence. Dementia risk, cognitive decline, mortality, and cardiometabolic burden all pointed toward age-linked vulnerability.
Those outcomes are not interchangeable, but they make the same broad argument: schizophrenia is not confined to hallucinations, delusions, or cognition alone.
Telomeres and Stress Biology Were More Consistent Than Epigenetic Clocks
Telomeres are protective chromosome caps that tend to shorten with cell division and stress. Across four meta-analyses, schizophrenia was associated with shorter telomere length, with effect sizes around -0.4 to -0.5.
Other body-wide systems also appeared repeatedly:
- Oxidative stress: cellular damage pathways that can accumulate with aging and illness burden.
- Inflammation: immune activity that may connect psychiatric symptoms with cardiometabolic risk.
- Mitochondrial function: energy-production biology relevant to brain and body resilience.
- IGF-1 signaling: a growth-factor pathway tied to metabolism and aging biology.
Epigenetic clocks were more mixed. Some showed modest acceleration, while others were neutral or even decelerated in early-stage cohorts.
That inconsistency is one reason the review avoids a simplistic “everything ages faster” conclusion.
Telomere shortening and oxidative or inflammatory stress looked more consistent than epigenetic clock acceleration.
The biology appears real, but it is not a single clock running hot across every tissue and every method.
Biological-age tools can overcompress a complex illness into one number. The review argues for a more cautious view.
Aging markers matter most when tied to specific mechanisms, tissues, and clinical outcomes.
First-Episode Findings Weaken the Lifestyle-Only Explanation
A common objection is that aging markers in schizophrenia may be caused by long-term antipsychotic exposure, smoking, inactivity, poverty, or fragmented medical care.
Those factors matter, but they cannot explain every finding.
The review highlights evidence from minimally treated and first-episode cohorts showing early biological differences. That does not remove confounding.
It suggests the aging phenotype may be partly embedded in the illness biology rather than entirely produced by treatment or lifestyle.
At the same time, the review does not let confounding off the hook. Antipsychotic exposure, metabolic disease, smoking, sleep disruption, trauma, social adversity, and healthcare access can all shape aging markers.
- Treatment exposure: antipsychotic history and metabolic side effects can alter downstream risk.
- Lifestyle burden: smoking, sleep disruption, inactivity, and poverty can worsen aging markers.
- Care access: fragmented medical treatment can let cardiovascular and metabolic problems compound.
The hard question is how these forces interact with the disease process rather than which one deserves all the blame.
Telomeres and BrainAGE Are Not Clinic-Ready Tests
This review does not prove that clinicians should order telomere tests or brain-age scans for patients. These tools remain research measures, and the validity of biological-age proxies in severe mental illness is still uncertain.
The clinical implication is broader. Schizophrenia care should not treat cardiometabolic, cognitive, immune, and aging-related risks as side issues.
They may be part of the same multisystem phenotype.
That framing supports earlier prevention. If aging-related risk is already detectable near first episode, waiting decades to address cardiovascular health, inflammation, cognition, sleep, and metabolic dysfunction is a bad strategy.
The body-wide consequences are not late add-ons.
It also changes how research should measure outcomes. A treatment that improves psychosis symptoms but worsens metabolic or inflammatory risk may be less successful than it looks.
Long-term function depends on the whole system.
Advanced Aging Fits Better Than a Runaway Clock
The review argues that “advanced aging” may be more accurate than “accelerated aging” in many contexts. The phrase is less dramatic, but better matched to the evidence.
It captures early biological deviation without assuming every aging marker worsens faster over time.
The conceptual shift is broad. Schizophrenia may involve thought, perception, and dopamine signaling while also altering systemic resilience.
Inflammation, oxidative stress, telomere maintenance, brain structure, and metabolic aging all moved in the wrong direction earlier than expected.
- Brain-age estimates: many studies found brains that looked several years older than chronological age.
- Telomere findings: chromosome-end markers were consistently shorter across meta-analyses.
- Body-wide systems: inflammation, oxidative stress, metabolism, and cardiometabolic risk repeatedly pointed beyond a brain-only model.
The next generation of studies will need longitudinal designs, better control of medication and lifestyle factors, and multi-omics measures that can separate cause from consequence.
The review does not solve cause and effect, but it makes the old brain-only frame too small.
For patients and families, the message should not be fatalistic. Advanced biological aging is not destiny.
It is evidence that prevention, metabolic care, sleep, exercise, smoking cessation, social support, and inflammation-related research should be treated as core parts of schizophrenia care rather than wellness extras.
The aging hypothesis is most clinically relevant when it avoids fatalism. It argues that the illness touches systems clinicians can monitor and, in some cases, modify earlier than they usually do.
The phrase “advanced aging” is less flashy than “accelerated aging,” but it is probably more actionable. It points to an early biological offset that should be measured, tracked, and treated as part of serious mental illness care.
Citation: DOI: 10.1192/bjp.2026.10606. Fernandez-Egea et al. Schizophrenia and accelerated aging: systematic review and future research directions. The British Journal of Psychiatry. 2026;1-13.
Study Design: Systematic review of aging markers in schizophrenia and non-affective psychosis.
Sample Size: 170 studies included from 923 manuscripts screened, covering brain imaging, cognition, telomeres, inflammation, metabolism, and mortality-related measures.
Key Statistic: Most studies were moderate or high quality: 93 of 170 were rated high quality and 75 were rated moderate quality.
Caveat: The evidence spans heterogeneous measures and remains vulnerable to medication, lifestyle, healthcare-access, and illness-severity confounding.