TL;DR: Diabetes and depression form a vicious cycle: high blood sugar triggers neuroinflammation and HPA axis dysfunction that cause depression, while depression sabotages blood sugar control through behavioral and metabolic pathways.
Doctors have known for years that depression and type 2 diabetes often occur together. A patient in the clinic with uncontrolled blood sugar frequently reports low mood, anxiety, and loss of interest. But the relationship isn’t simply coincidence or shared risk factors.
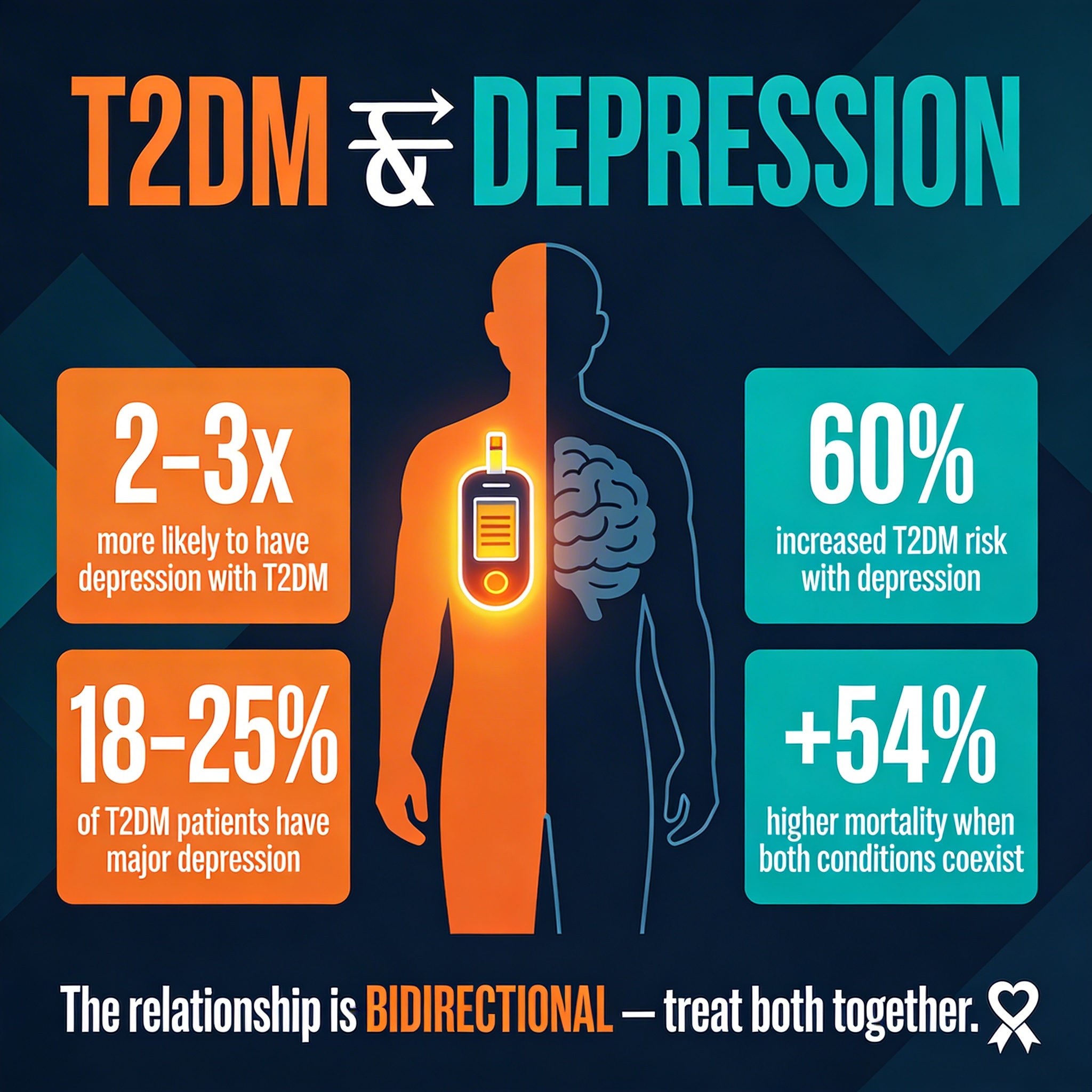
New evidence reveals a vicious cycle: diabetes triggers depression and anxiety through inflammatory and hormonal pathways in the brain, and depression and anxiety, in turn, increase the risk of developing or worsening diabetes. This bidirectional connection creates a trap where treating one disease without addressing the other leaves patients in a downward spiral.
Understanding these mechanisms—and the behavioral and biological links between them—is essential for integrated care.
Key Findings
- Odds ratios 1.12–1.15: People with depression and anxiety have a significantly elevated risk of developing type 2 diabetes; Mendelian randomization analysis found odds ratios of 1.12 (95% CI 1.07–1.39, p = 0.002) for depression and 1.15 (95% CI 1.02–1.31, p = 0.02) for anxiety.
- Bidirectional risk: Individuals with type 2 diabetes show higher rates of depression and anxiety than non-diabetic controls, with long-term hyperglycemia and poor glycemic control exacerbating mood disturbances.
- Neuroinflammation pathway: Hyperglycemia-induced inflammation (elevated high-sensitivity C-reactive protein and proinflammatory cytokines) crosses the blood-brain barrier and disrupts hippocampal function, a key site for mood and memory regulation.
- HPA axis dysregulation: Chronic hyperglycemia activates the hypothalamus-pituitary-adrenal (HPA) axis, elevating cortisol levels and impairing negative feedback control, creating a state of chronic psychological stress that mirrors depression.
- Lifestyle sabotage: Behavioral mechanisms link depression and anxiety to diabetes progression: depressed individuals show reduced physical activity, poorer medication adherence, increased smoking, and higher body mass index—all risk factors for poor glycemic control.
- Glucose variability matters: At clinically relevant fasting plasma glucose (FPG) levels and glycosylated hemoglobin (HbA1c) elevations, both baseline hyperglycemia and glucose variability independently predict depression and anxiety symptoms.
Source: Journal of Affective Disorders (2025) | Xu & Chen | The bidirectional influence between type 2 diabetes mellitus and the state of depression and anxiety.
The Problem Within the Problem: Comorbidity as Causality
The relationship between diabetes and depression isn’t simple comorbidity. Large prospective studies show that depressed people are measurably more likely to develop diabetes, and diabetic people are more likely to develop depression. It’s a bidirectional loop.
For decades, this pattern was filed under “comorbidity”—a polite term meaning “we don’t fully understand why they occur together.” But Xu and Chen’s comprehensive review reveals something far more troubling: it’s not comorbidity. It’s bidirectional causality.
The evidence converges from multiple angles. Prospective cohort studies following 167,729 subjects over 9 years show that depressed and anxious people are more likely to develop diabetes, even after controlling for obesity and smoking. Mendelian randomization studies—which use genetic variants to infer causal direction—confirm that psychiatric disorders causally increase diabetes risk.
Longitudinal studies of diabetic populations show that depression and anxiety actually worsen glycemic control and accelerate diabetes progression. Each condition exacerbates the other, trapping patients in a spiral that treating either disease alone rarely breaks.
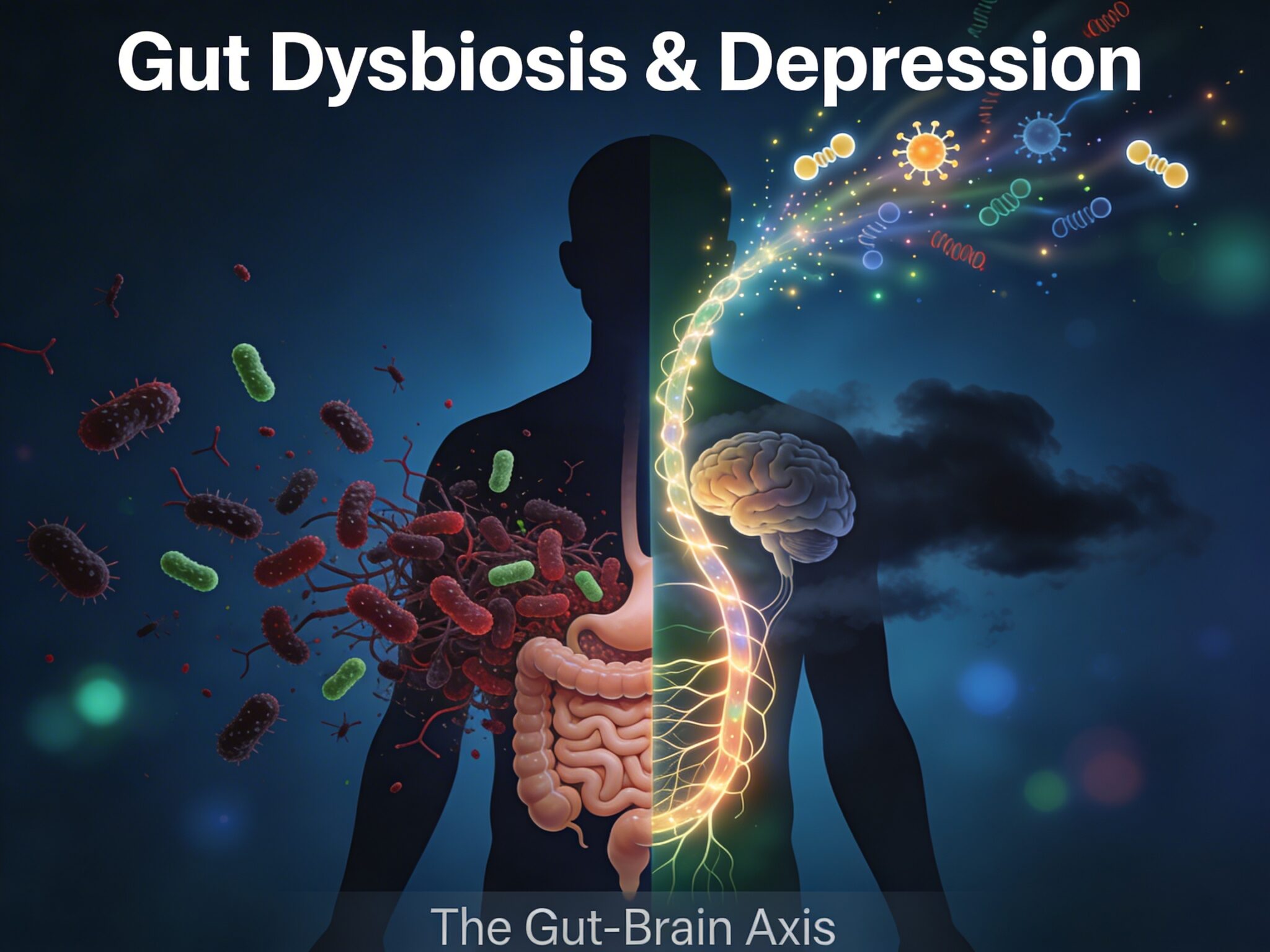
The Inflammatory Bridge: How Blood Sugar Breaks into the Brain
How does high blood sugar create mood disturbance? The first pathway is inflammation. Prolonged hyperglycemia drives oxidative stress and activates immune cells in adipose tissue and liver, releasing a cascade of proinflammatory mediators:
- TNF-alpha, IL-6, IL-1 beta: Key proinflammatory cytokines released from adipose tissue and liver.
- C-reactive protein: Elevated in prolonged hyperglycemia, crosses the blood-brain barrier especially when the barrier is compromised by chronic inflammation.
- Microglial activation: Once these molecules enter the brain, they interact with microglial cells—the brain’s resident immune sentries—triggering neuroinflammation.
This process is particularly damaging in the hippocampus, the brain region essential for memory and mood regulation. Neuroinflammation there impairs synaptic plasticity and reduces brain-derived neurotrophic factor (BDNF), a growth factor crucial for neural survival and resilience.
The result: a hyperglycemic patient whose brain is chronically inflamed, whose mood circuits are weakened, and whose memory and motivation suffer. C-reactive protein levels are significantly associated with depression and anxiety in diabetic populations—establishing inflammation as a measurable bridge between blood glucose and mental state.
Stress Hormones and the HPA Axis Trap
A second mechanism involves the hypothalamus-pituitary-adrenal (HPA) axis, the body’s central stress-response system. Hyperglycemia activates this axis, chronically elevating cortisol—the stress hormone. In normal physiology, cortisol is released in response to acute threats and then suppressed by negative feedback.
But chronic hyperglycemia keeps the spigot open. The brain, flooded with cortisol, loses its ability to shut the system down. The hippocampus, packed with glucocorticoid receptors, bears the brunt.
Chronically elevated cortisol damages hippocampal neurons, reduces neurogenesis, and impairs the negative feedback loops that normally constrain the HPA axis. The result is chronic HPA hyperactivity that, neurobiologically, is indistinguishable from clinical depression.
This is why depression so often emerges with poor glycemic control. The body has no mechanism to distinguish between a stalking predator and a fasting glucose of 250 mg/dL. Both activate the HPA axis. Both trigger cortisol release. Both, if prolonged, damage the hippocampus.
Depression in diabetes is not demoralization—it’s a biological consequence of sustained metabolic stress.
Neurotransmitter Deficiency: The Missing Chemistry
A third pathway involves neurotransmitter dysfunction. Type 2 diabetes damages small blood vessels supplying the brain, reducing perfusion and impairing the synthesis of key neurotransmitters—dopamine, norepinephrine, and serotonin (5-HT)—all essential for mood, motivation, and pleasure.
Hyperglycemia-induced oxidative stress can also directly damage the enzymes that produce these neurotransmitters. The consequence: a brain starved of the very molecules that drive emotional stability. A depressed diabetic patient isn’t just sad—they’re chemically depleted.
Insulin itself has neuroprotective functions beyond glucose control. It facilitates serotonin synthesis and shields neurons from oxidative damage. In advanced type 2 diabetes, insulin resistance impairs these protective effects—another pathway from metabolic dysfunction to mood disruption.
The Behavioral Downward Spiral: When Depression Sabotages Diabetes Management
But hyperglycemia doesn’t just cause depression. Depression, in turn, sabotages diabetes management through behavioral mechanisms. Depression impairs the very behaviors essential for glycemic control:
- Physical activity: Depressed individuals exercise significantly less.
- Diet quality: Eating patterns become less healthy.
- Substance use: Increased smoking and excessive alcohol use.
- Medication adherence: Reduced adherence to medication and blood glucose monitoring.
Large prospective studies—including one tracking 2,981 subjects over 2 years—found that depression and anxiety increased diabetes risk from 1.6% to 2.5%, with much of the effect mediated by these lifestyle changes: reduced physical activity, weight gain, and smoking.
Depression also impairs executive function and decision-making—precisely the capacities needed for diabetes self-management: insulin dosing, carbohydrate counting, blood glucose interpretation.
A depressed patient struggles with cognitive clarity and concentration. This makes adherence harder, further worsening glycemic control and intensifying HPA axis stress. The system cascades downward.
Toward Integrated Care: Breaking the Cycle
The clinical implication is stark: treating diabetes without screening for mood disturbance is incomplete medicine. Treating depression while ignoring glycemic control leaves patients vulnerable to neurobiological relapse driven by ongoing hyperglycemia.
Depression in diabetes is not poor coping—it’s metabolic dysfunction reaching the brain. Poor glycemic control in depression is not laziness—it’s neurobiological impairment. Recognizing these causal links changes how both conditions should be managed.
The evidence points to multimodal interventions. Physical activity improves both mood (through dopamine and BDNF) and glycemic control. Stress reduction and sleep optimization lower cortisol and HPA axis activation.
Anti-inflammatory dietary patterns may reduce both systemic and neuroinflammation. Medications for mood or glucose control need to be chosen with both conditions in mind, avoiding agents that worsen one while treating the other.
The Missing Link: Why Prevention Matters
Perhaps the most important implication is preventive. If depression and anxiety causally increase diabetes risk, then screening for and treating mood disorders in high-risk populations is a form of diabetes prevention.
Conversely, aggressive glycemic control in early diabetes may prevent depression and anxiety from ever emerging. The window of intervention is there—early, before the bidirectional trap fully closes.
Blood sugar affects the brain. The brain affects glucose control. Inflammation in the periphery ignites inflammation in the mind. These are not separate diseases that happen to coexist—they are linked, each fueling the other. Understanding this bidirectionality is the first step toward breaking free.
Full Citation:
Xu, H., & Chen, Q. (2025). The bidirectional influence between type 2 diabetes mellitus and the state of depression and anxiety. Journal of Affective Disorders, 386, 119467. DOI: 10.1016/j.jad.2025.119467
Affiliations: Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, China.
Note: This is a comprehensive review article synthesizing evidence from multiple clinical trials, cohort studies, Mendelian randomization analyses, and mechanistic studies conducted across numerous international research centers.