Obesity and Depression Share Five Converging Biological Pathways
Obesity and depression represent two of the world’s fastest-growing epidemics. By 2030, over 1 billion people will have obesity, while depression will affect more than 350 million. Yet they are rarely treated together despite overwhelming evidence they are mechanistically linked. Epidemiological data reveal a striking bidirectional relationship: obese individuals have a 55% higher lifetime risk of developing depression, while those with depression have a 58% higher risk of becoming obese. In obese populations, depression prevalence reaches approximately 30%—three times the rate in people of normal weight. This is not coincidence. Five interconnected biological pathways—chronic inflammation, neuroendocrine dysregulation, metabolic hormone resistance, lipid-driven neuronal toxicity, and gut dysbiosis—create a self-amplifying cycle where each condition worsens the other. Breaking this cycle requires integrated treatment addressing all pathways simultaneously, not isolated management of either condition alone.
Key Findings
- Obese individuals have 55% greater lifetime risk of depression; depressed individuals have 58% higher risk of obesity
- Depression prevalence in obese populations reaches approximately 30%, compared to 10% in normal-weight populations—a three-fold difference
- Five convergent mechanisms link the conditions: chronic visceral inflammation (TNF-α, IL-6, CRP), HPA axis dysregulation with glucocorticoid resistance, loss of metabolic hormone signaling (leptin, insulin, adiponectin) and BDNF production, accumulation of toxic lipids and ceramides within neurons, and dysbiosis-driven reduction of mood-supporting bacterial metabolites
- Visceral adipose tissue actively releases pro-inflammatory cytokines that cross the blood-brain barrier and activate microglia, triggering neuroinflammation and suppressing serotonin synthesis
- Dysbiotic gut bacteria reduce production of short-chain fatty acids and neurotransmitters (GABA, serotonin dopamine) while increasing bacterial lipopolysaccharide translocation, amplifying brain inflammation
- Integrated interventions addressing multiple pathways simultaneously (diet, exercise, microbiota optimization) show greater efficacy than single-target approaches
Source: International Journal of Molecular Sciences (2025) | Monsalve et al.
Visceral Inflammation Activates Brain Immune Cells and Suppresses Mood Neurotransmitters
Deep abdominal fat (visceral adipose tissue) is metabolically distinct from subcutaneous fat. Visceral adipocytes continuously release pro-inflammatory cytokines including tumor necrosis factor alpha (TNF-α), interleukin 6 (IL-6), and C-reactive protein (CRP). These molecules circulate systemically and importantly, cross the blood-brain barrier through both paracellular diffusion and active transport mechanisms. Once in the brain, inflammatory cytokines encounter resident innate immune cells called microglia.
Microglial activation in response to circulating inflammatory signals triggers a cascade of neurobiological changes. Activated microglia release additional cytokines, chemokines, and free radicals within the brain parenchyma. This neuroinflammation directly suppresses serotonin synthesis in the raphe nuclei, reduces neurotrophic support (BDNF) needed for hippocampal neurogenesis, and damages synaptic connections through complement-mediated synaptic pruning. The process is bidirectional: depression itself elevates circulating inflammatory markers through heightened HPA axis activity and enhanced cellular stress responses, creating a self-perpetuating inflammatory cycle.
HPA Axis Dysregulation: Stress Hormones Drive Visceral Fat Accumulation and Depression
The hypothalamic-pituitary-adrenal (HPA) axis is the body’s primary neuroendocrine stress response system, controlled by corticotropin-releasing hormone (CRH) and regulated by glucocorticoid feedback inhibition via cortisol. In obesity, this system malfunctions. Elevated cortisol chronically signals the body to preferentially store calories as visceral (abdominal) fat while simultaneously suppressing energy expenditure. Cortisol also increases appetite, particularly for calorie-dense foods, perpetuating weight gain.
Critically, the chronic low-grade inflammation present in obesity blunts glucocorticoid receptor function—a state called glucocorticoid resistance. Inflammatory molecules interfere with cortisol’s ability to properly signal cellular glucocorticoid receptors, preventing normal negative feedback inhibition of the HPA axis. The result is an overactive yet dysregulated HPA axis: cortisol levels remain elevated despite maximal feedback inhibition attempts, and this sustained hypercortisolism directly contributes to depression by disrupting monoamine synthesis, increasing glutamate excitotoxicity, and suppressing hippocampal neuroplasticity.
Metabolic Hormone Resistance: Loss of BDNF and Neuronal Growth Signals
Obesity triggers resistance to leptin and insulin—hormones normally produced in response to energy stores. Leptin is released by adipose tissue in proportion to fat mass; under healthy conditions, it signals the hypothalamus to reduce hunger and increase energy expenditure. Insulin is secreted by pancreatic beta cells after meals to regulate blood glucose; it also has neuroendocrine effects in the brain. Both leptin and insulin stimulate production of brain-derived neurotrophic factor (BDNF), a critical growth factor supporting neuronal survival, synaptic plasticity, and neurogenesis.
In obesity, leptin and insulin resistance develop—the brain becomes less responsive to these hormones. As a consequence, BDNF production in the prefrontal cortex and hippocampus plummets. Without adequate BDNF, neurons cannot grow, establish new synaptic connections, or recover from inflammatory damage. Concurrently, adiponectin—an adipokine released by fat tissue that supports neuronal health and mitochondrial function—is reduced in obesity. The net result is a state of nutritional deprivation in the brain despite systemic caloric excess. Neurons are simultaneously exposed to high inflammatory cytokines (which damage them) and deprived of growth factors (which would help them repair). Depression itself worsens this state by further suppressing leptin signaling and BDNF production, deepening the metabolic-neurological deficit.
Lipid Toxicity and Mitochondrial Dysfunction: Cellular Energy Crisis in Neurons
In obesity, elevated circulating free fatty acids and dysregulated lipid metabolism lead to accumulation of lipids not just in storage tissues but within neurons and glial cells. Saturated fatty acids and their metabolic derivatives, particularly ceramides (bioactive lipids formed from sphingosine and fatty acyl-CoA), are especially neurotoxic. Ceramides accumulate within neuronal mitochondria and endoplasmic reticulum, directly damaging the structural integrity of these organelles.
Damaged mitochondria produce less ATP—the cellular energy currency—and simultaneously generate excessive amounts of reactive oxygen species (free radicals) through impaired electron transport chain function. In neurons, which are among the most metabolically active cells in the body, this energy deficit is catastrophic. Neurons cannot sustain the energetically expensive processes required for mood regulation: neurotransmitter synthesis and vesicular release, maintenance of ion gradients, receptor trafficking, synaptic remodeling, and antioxidant defenses. Additionally, ceramides trigger additional neuroinflammatory signaling pathways. The brain effectively enters a state of cellular energy crisis—neuroinflammation increases metabolic demands while mitochondrial dysfunction reduces ATP production. This energetic failure explains why depression increasingly appears to be a disorder of cellular bioenergetics in brain regions supporting emotion and cognition.
Dysbiosis: How Dysbiotic Bacteria Amplify Brain Inflammation and Reduce Mood Support
Obesity systematically alters the composition of the gut microbiota (dysbiosis). Under healthy conditions, the microbiota is populated by bacteria producing short-chain fatty acids (SCFAs), particularly butyrate, which strengthen the intestinal epithelial barrier and reduce microbial translocation. Additionally, healthy commensal bacteria produce neurotransmitters including GABA, serotonin, and dopamine precursors that influence brain function through the vagus nerve and systemic circulation.
In obesity, dysbiosis develops: beneficial bacteria that produce SCFAs decline (reductions in Faecalibacterium prausnitzii, Roseburia spp., and Akkermansia muciniphila), while pathogenic gram-negative bacteria flourish. The dysbiotic microbiota produces fewer SCFAs and neurotransmitters, depriving the brain of microbial metabolites that support mood. Simultaneously, the dysbiotic state damages the intestinal epithelial barrier, creating “leaky gut.” Bacterial lipopolysaccharides (LPS)—endotoxins from gram-negative bacterial cell walls—translocate across the compromised barrier into the bloodstream. These endotoxins circulate to the brain, where they activate toll-like receptors on microglia and trigger intense neuroinflammation.
The dysbiotic state also alters tryptophan metabolism. Healthy bacteria help convert tryptophan into serotonin-precursor molecules and other neuroprotective metabolites. Dysbiotic bacteria shunt tryptophan toward the kynurenine pathway, producing metabolites (particularly quinolinic acid) that are neurotoxic, suppress mood, and exacerbate neuroinflammation. This tryptophan dysmetabolism directly reduces brain serotonin synthesis, contributing to depressive symptoms. Depression itself alters the microbiota through stress-hormone effects on bacterial growth, changes in eating patterns, sleep disruption, and altered bile acid metabolism—creating a bidirectional cycle where depression perpetuates dysbiosis and dysbiosis perpetuates depression.
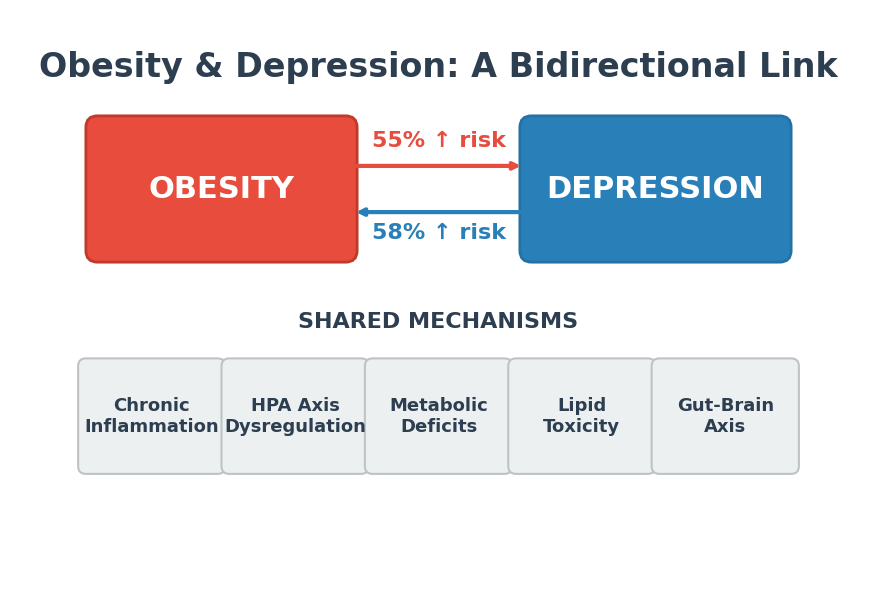
Image file: obesity-depression-risk.png — Bidirectional risk relationship: obese individuals have 55% increased depression risk; those with depression have 58% increased obesity risk (epidemiological data)
The Self-Perpetuating Cycle: How Each Condition Drives the Other Forward
These five pathways do not operate in isolation—they form an interconnected web where each amplifies the others. Consider the cascade: initial modest weight gain triggers low-level chronic inflammation and mild HPA axis dysregulation. This neuroinflammation suppresses mood neurotransmitters, triggering early depression symptoms. Depression reduces physical activity and worsens sleep quality, which shifts dietary patterns toward processed, high-calorie foods and disrupts circadian regulation of metabolism. Poor diet and disrupted sleep reshape the microbiota (dysbiosis), which reduces production of protective short-chain fatty acids and neurotransmitters while increasing bacterial endotoxin translocation. Increased brain inflammation from circulating LPS and reduced BDNF signaling deepen depression. Lower motivation for exercise and activity-avoidance behaviors in depression promote further visceral fat accumulation. Metabolic hormone resistance develops, reducing BDNF production further. Mitochondrial damage from accumulated lipids and ceramides compounds the cellular energy crisis. What began as modest weight gain becomes severe obesity alongside major depression, each condition recursively driving the other forward into a pathological steady state.
Breaking the Cycle Requires Multi-Pathway Interventions
Why single-target approaches fail: Because obesity and depression are linked through five converging pathways, treating only one condition in isolation rarely succeeds. Weight loss programs that do not address inflammation and depression show high relapse rates; patients regain weight because the underlying neurobiological drivers (inflammation, dysbiosis, BDNF deficiency) remain. Antidepressants without metabolic intervention fail to prevent weight gain and often promote it through both pharmacological effects (appetite stimulation) and behavioral mechanisms (reduced motivation for activity). Integrated approaches targeting multiple pathways simultaneously show substantially greater efficacy.
Anti-inflammatory diet and aerobic exercise address all five pathways: Exercise is among the most powerful multi-pathway interventions available. Aerobic activity reduces visceral fat accumulation, decreases circulating inflammatory cytokines (TNF-α, IL-6, CRP), restores HPA axis sensitivity to glucocorticoid feedback, normalizes leptin and insulin signaling, increases BDNF production in the prefrontal cortex and hippocampus, improves mitochondrial oxidative capacity, and remodels the microbiota toward beneficial short-chain fatty acid-producing bacteria. Mediterranean-style and high-fiber diets reduce bacterial endotoxin translocation, improve microbial diversity, increase short-chain fatty acid production, and reduce systemic inflammation. Both interventions address visceral inflammation, HPA dysregulation, metabolic hormone resistance, mitochondrial dysfunction, and dysbiosis simultaneously.
Optimize gut health through targeted microbiota interventions: Dietary fiber, resistant starch, and prebiotic compounds promote growth of beneficial bacteria. Specific probiotic strains show promise for both obesity and depression—for example, Akkermansia muciniphila supplementation improves intestinal barrier integrity and reduces inflammatory markers. Fermented foods, polyphenol-rich foods (berries, tea, wine), and omega-3 polyunsaturated fatty acids all shift microbiota composition toward mood-supporting genera. In select cases, fecal microbiota transplantation has been explored for severe dysbiosis resistant to dietary intervention.
Screen both conditions systematically in clinical settings: Patients with obesity should be routinely screened for depression using validated instruments (PHQ-9, or structured clinical interview). Patients presenting with depression should be evaluated for metabolic syndrome (including visceral obesity, insulin resistance, dyslipidemia, hypertension) and dysbiosis markers (stool microbiota analysis, fecal calprotectin). The goal is early detection before the obesity-depression cycle becomes entrenched. This requires collaboration between primary care, psychiatry, gastroenterology, and endocrinology.
Use biomarkers to guide personalized intervention: Blood inflammatory markers (CRP, IL-6, TNF-α) reveal the degree of systemic and neuroinflammation; individuals with marked inflammation may benefit especially from anti-inflammatory dietary and pharmacological interventions. Insulin resistance and BDNF levels indicate metabolic and neurotrophic deficiency severity. Fecal microbiota composition and serum lipopolysaccharide-binding protein reveal dysbiosis severity and endotoxemia. Oxidative stress markers indicate mitochondrial dysfunction. These biomarkers can guide treatment selection—identifying which pathway dominates in each individual and prioritizing interventions targeting the most dysregulated systems.
The Research Foundation: Multi-Pathway Evidence Integration
This analysis synthesizes evidence from thousands of mechanistic studies, clinical trials, and epidemiological investigations published over the past two decades. The 2025 International Journal of Molecular Sciences review by Monsalve et al. comprehensively integrated this evidence, demonstrating that obesity and depression share converging biological pathways involving visceral adipose tissue-derived inflammation, HPA axis dysregulation, metabolic hormone resistance (leptin, insulin, adiponectin), lipid-derived neurotoxicity, and dysbiosis-driven changes in the microbiota-gut-brain axis. The reviewers emphasize that effective treatment must address this integrated pathophysiology rather than continuing to treat obesity and depression as separate siloed conditions.
Clinical and Public Health Implications
With over 1 billion people predicted to have obesity and 350+ million with depression by 2030, the obesity-depression connection is a major public health priority. Current healthcare systems often maintain separate obesity clinics, psychiatry services, and primary care—missing the fundamental biology linking these conditions. Recognizing obesity and depression as manifestations of the same dysregulated biological systems could reshape clinical training, service organization, and treatment outcomes.
Prevention starting in childhood is critical. School-based programs addressing diet quality, physical activity, sleep hygiene, stress management, and social connection can prevent both obesity and depression. Community interventions that improve food environments (reducing ultra-processed foods, improving access to fruits and vegetables), increase opportunities for movement (walkable neighborhoods, parks, community sports), and enhance green space exposure address all five pathways simultaneously. Such preventive approaches could interrupt the obesity-depression cycle before it becomes pathologically entrenched.
Citation: Monsalve, F. A., Fernández-Tapia, B., Arriagada, O. C., González, D. R., & Delgado-López, F. (2025). Obesity and depression: A pathophysiotoxic relationship. International Journal of Molecular Sciences, 26(23), 11590. doi:10.3390/ijms262311590
Authors’ affiliations: Department of Preclinical Sciences, Faculty of Medicine, Universidad Católica del Maule, Chile; Nursing School, Faculty of Health Sciences, Universidad de Talca, Chile; Department of Basic Biomedical Sciences, Faculty of Health Sciences, Universidad de Talca, Chile; Biomedical Research Laboratory, Department of Preclinical Sciences, Faculty of Medicine, Universidad Católica del Maule, Chile.