TL;DR: A 2026 study in Journal of Clinical Sleep Medicine found that in 65 continuous positive airway pressure (CPAP) adherent patients with obstructive sleep apnea, those who still showed objective daytime sleepiness on a psychomotor vigilance task scored worse on global cognition, memory, executive function, attention, and processing speed despite using their devices regularly.
Key Findings
- 65 adherent CPAP users still split into sleepy and non-sleepy groups: All participants averaged at least 6 hours of PAP use per night and had device-reported normalized apnea-hypopnea indices, yet 46% still met objective excessive daytime sleepiness criteria on the Psychomotor Vigilance Task.
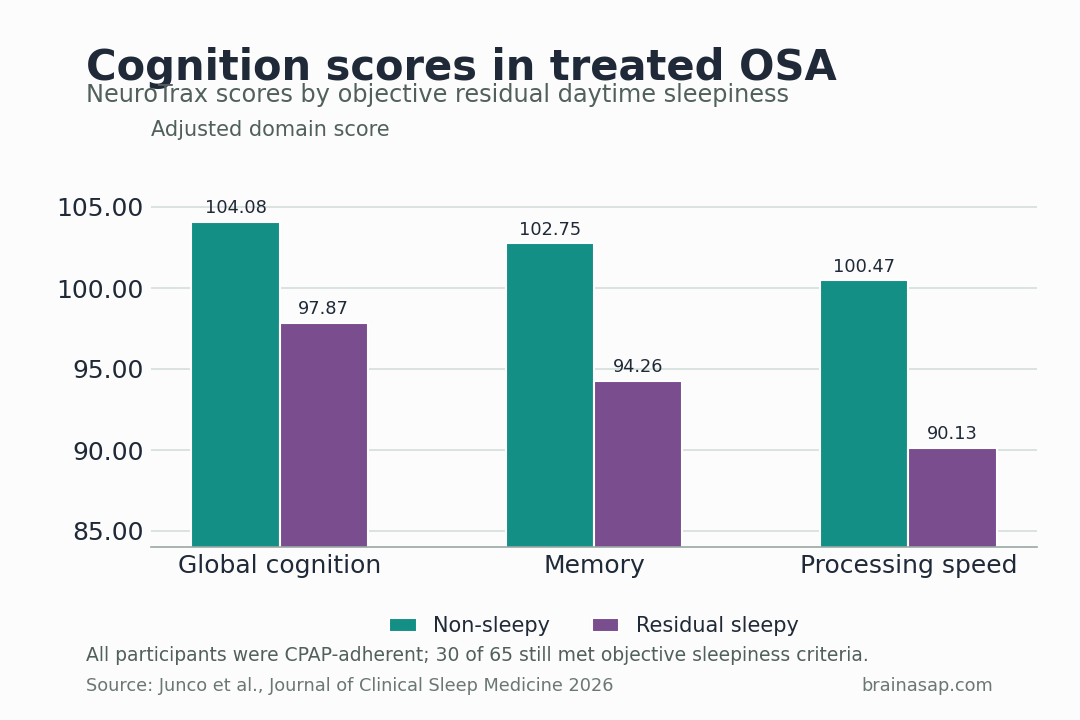
- Global cognition fell from 104.08 to 97.87 with residual sleepiness: After adjustment, participants with objective daytime sleepiness performed significantly worse on overall cognition (p = 0.033).
- Memory dropped even more sharply: The sleepy group scored 94.26 on memory versus 102.75 in the non-sleepy group, with an adjusted group difference of about 8.77 points and p = 0.002.
- More vigilance lapses predicted broader cognitive weakness: Higher lapse counts were linked to worse global cognition (β = -4.09), memory (β = -3.97), executive function (β = -3.91), attention (β = -2.68), and processing speed (β = -4.89).
- Subjective sleepiness missed the problem: Epworth Sleepiness Scale scores did not differ meaningfully between groups, and the correlation between ESS and PVT lapses was near zero (rho = 0.021, p = 0.876).
Source: Journal of Clinical Sleep Medicine (2026) | Junco et al.
One of the most misleading ideas in sleep medicine is that once CPAP use looks good on the machine report, the brain side of sleep apnea is basically fixed.
This study argues that residual daytime sleepiness may mark a distinct cognitive-risk phenotype that survives even after airflow metrics normalize.
Why a Normal CPAP Download Does Not Guarantee a Normal Brain Day
Sleep clinics are very good at measuring breathing. Study details:
They are less good at measuring next-day vigilance and cognition. That mismatch is what makes residual excessive daytime sleepiness in obstructive sleep apnea so clinically important.
A patient can use positive airway pressure faithfully, bring the device-reported apnea-hypopnea index below 5, and still move through the day cognitively dulled.
If that residual sleepiness tracks memory and attention deficits, it means successful breathing treatment and successful brain recovery are not always the same outcome.
The MAGNETO study was designed around exactly that problem.
Rather than asking whether untreated sleep apnea hurts cognition, it focused on a more difficult group: patients who were already doing what they were supposed to do with therapy.
What a 65-Patient Treated OSA Cohort Could Show That Older Studies Missed
The cohort included 65 PAP-adherent adults with obstructive sleep apnea.
Average nightly use was about 6.9 hours, all participants had normalized residual AHI on their devices, and the sample was not demographically generic: mean age was 61, 72% identified as Hispanic or Latino, and nearly half had severe OSA at diagnosis.
Instead of relying on self-report alone, researchers used the Psychomotor Vigilance Task, or PVT, as their objective sleepiness measure.
More than five lapses of 500 milliseconds or longer counted as residual daytime sleepiness.
By that standard, 30 of the 65 participants, or 46%, still qualified as sleepy despite adequate PAP adherence.
That alone is worth noticing. Residual sleepiness is not a rare leftover. It is common enough to look like a real phenotype inside treated OSA rather than a clinical oddity.
The Most Important Result Is the Gap Between PVT and Epworth Scores
One of the sharpest findings in the paper is that subjective sleepiness barely tracked the objective measure.
Epworth Sleepiness Scale scores were similar between groups, and the correlation between ESS and PVT lapses was essentially nonexistent: rho = 0.021 with p = 0.876.
The reason is it means many patients who look “not that sleepy” on a questionnaire can still have measurable vigilance failure.
If clinicians only ask how sleepy someone feels, they may miss the subgroup whose cognition is taking a hit even while subjective symptoms appear mild.
The authors’ framing is persuasive here.
Residual EDS may be less a complaint and more a cognitive risk marker.
Patients are not always the best sensors of their own vigilance instability, especially when the impairment has become their new normal.
How Residual Sleepiness Showed Up in Global Cognition, Memory, and Processing Speed
The categorical comparison is straightforward. Participants with residual daytime sleepiness scored 97.87 on global cognition versus 104.08 in the non-sleepy group.
Memory showed an even larger split: 94.26 versus 102.75. Information processing speed also lagged, at 90.13 versus 100.47.
After adjustment for sex, time since diagnosis, and self-reported sleep duration, the sleepy group still performed significantly worse on global cognition and memory.
The adjusted difference worked out to about 6.41 points for global cognition and 8.77 points for memory, or roughly 0.43 to 0.58 standard deviations on the NeuroTrax scale.
The continuous models widened the result. More total PVT lapses predicted weakness across multiple domains:
- Global cognition and memory: β = -4.09 and β = -3.97, respectively.
- Executive function and attention: β = -3.91 and β = -2.68, respectively.
- Processing speed: β = -4.89, the largest continuous-domain estimate.
Slower average reaction time showed a similar pattern. Reaction-time variability, by contrast, largely dropped out after false-discovery-rate correction.
Residual Sleepiness Marked a Brain Health Phenotype, Not Just a Sleep Complaint
These findings fit a growing idea in sleep medicine: treated OSA is not one biological endpoint. 2 patients can both appear “controlled” on PAP metrics while only one remains cognitively vulnerable.
That vulnerability may matter far beyond daytime functioning.
The paper situates residual EDS inside a larger literature linking sleepiness to cognitive decline and dementia risk.
The authors are careful not to overclaim, but their interpretation is sensible: the PVT can offer a quick way to detect the subgroup whose brain health remains at risk even after breathing appears fixed.
There is also a clinical lesson here for follow-up visits. A patient saying “I’m using my CPAP” is not enough.
A normal residual AHI is not enough either. If the person still drifts cognitively during the day, the treatment target has not really been met.
What CPAP Clinics Should Take From a 46% Residual Sleepiness Rate
The study is small, single-site, and cross-sectional, so it cannot prove causality.
It also cannot tell us whether reducing residual sleepiness would reverse the cognitive deficits.
But it raises a clinically uncomfortable test: how many “successfully treated” OSA patients are still carrying a meaningful cognitive burden that routine follow-up never measures?
The strongest answer from this paper is that objective vigilance testing belongs in the conversation.
The PVT is brief, cheap, and more revealing here than the Epworth Sleepiness Scale, which makes it attractive both for research and for clinics trying to spot patients who need more than adherence coaching.
If future studies confirm the pattern, residual EDS can become a triage marker for deeper evaluation: persistent sleep fragmentation, circadian issues, medication effects, depression, neurodegenerative vulnerability, or simply a subgroup whose brains remain especially sensitive to years of prior hypoxia and arousal burden.
In other words, this paper nudges sleep apnea care away from a narrow airway model and toward a brain-health model. CPAP may normalize breathing. It does not automatically normalize cognition.
The broader sleep-apnea picture has three practical layers:
- Breathing control: Positive airway pressure can normalize airflow metrics.
- Daytime cognition: Residual sleepiness can still track memory and attention problems.
- Clinical implication: Follow-up should ask how the patient functions during the day, not only what the device reports overnight.
Citation: DOI: 10.1007/s44470-026-00077-9. Junco et al. Cognition and psychomotor vigilance in treated sleep apnea patients with and without daytime sleepiness: the MAGNETO study. Journal of Clinical Sleep Medicine. 2026;22:60.
Study Design: Cohort study
Sample/Model: 65 adherent CPAP users still split into sleepy and non-sleepy groups: All participants averaged at least 6 hours of PAP use per night and had device-reported normalized apnea-hypopnea indices, yet 46% still met objective excessive daytime sleepiness criteria on the Psychomotor Vigilance Task.
Key Statistic: Global cognition fell from 104.08 to 97.87 with residual sleepiness: After adjustment, participants with objective daytime sleepiness performed significantly worse on overall cognition (p = 0.033).
Caveat: Single-study evidence; interpret with the source design and sample.