TL;DR: A 2026 study in NEJM Evidence found that solriamfetol added 9.4 minutes of objective wakefulness in early-morning shift work disorder after 4 weeks, without a higher overall adverse-event rate than placebo.
Key Findings
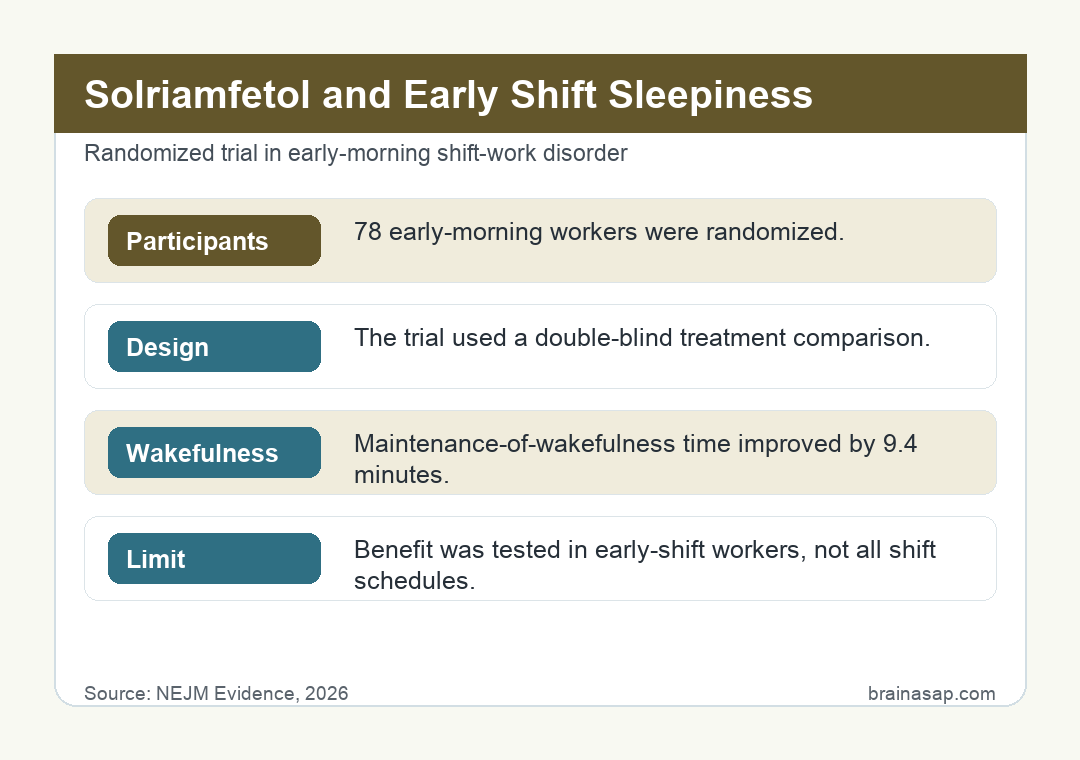
- 78 early-morning workers: Participants had excessive sleepiness linked to shifts starting between 3 a.m. and 7 a.m.
- Randomized double-blind design: The trial compared solriamfetol with placebo over 4 weeks.
- 9.4-minute wakefulness gain: Solriamfetol increased sleep latency on the Maintenance of Wakefulness Test by 9.4 minutes versus placebo (95% CI, 5.7 to 13.0; P<0.001).
- KSS improved by 1.2 points: Subjective sleepiness on the Karolinska Sleepiness Scale improved versus placebo (difference, -1.2; 95% CI, -1.7 to -0.7).
- Adverse events were common in both groups: Any adverse event occurred in 55% of solriamfetol-treated participants and 63% of placebo-treated participants; headache and nausea were most common.
Source: NEJM Evidence (2026) | Zitting et al.
Early-morning shift work disorder has a direct biological constraint: many workers start between 3 and 7 a.m., when the brain is still biased toward sleep.
Yet most medication research has focused on night-shift workers.
This NEJM Evidence trial targeted that overlooked schedule directly.
The Trial Focused on the Most Ordinary Bad Schedule
Night shifts get more research attention, but early starts may affect more people. A worker who clocks in at 4:30 a.m. may not identify as a shift worker at all.
Study details:
- 78 early-morning workers: Participants had excessive sleepiness linked to shifts starting between 3 a.m. and 7 a.m
- Randomized double-blind design: The trial compared solriamfetol with placebo over 4 weeks
- 9.4-minute wakefulness gain: Solriamfetol increased sleep latency on the Maintenance of Wakefulness Test by 9.4 minutes versus placebo (95% CI, 5.7 to 13.0; P<0.001)
- KSS improved by 1.2 points: Subjective sleepiness on the Karolinska Sleepiness Scale improved versus placebo (difference, -1.2; 95% CI, -1.7 to -0.7)
They may simply think they have an early job.
Biologically, that distinction is thin. Waking for a 3-to-7-in-the-morning start often means cutting sleep short during the circadian night, then trying to perform when alertness systems are not fully online.
The result can be sleepiness during work and difficulty getting enough sleep later.
The study tested solriamfetol, a selective dopamine and norepinephrine reuptake inhibitor already relevant to excessive sleepiness conditions, in the specific population that had been understudied.
9 Minutes on a Wakefulness Test Is Not Tiny
The primary endpoint was sleep latency on the Maintenance of Wakefulness Test: how long can someone stay awake under conditions designed to measure physiological sleepiness?
After 4 weeks, solriamfetol produced a 9.4-minute longer sleep latency than placebo. The trial’s efficacy readout had three helpful anchors:
- Objective wakefulness: sleep latency improved by 9.4 minutes versus placebo.
- Precision: the 95% confidence interval ran from 5.7 to 13.0 minutes.
- Statistical strength: the P value was below 0.001.
That does not show every worker felt transformed. But in a safety-critical context, such as driving, machinery, health care, or emergency response, a measurable increase in wakefulness can matter.
Subjective Sleepiness Moved in the Same Direction
Objective wakefulness is helpful, but people also care whether they feel less sleepy. The Karolinska Sleepiness Scale moved by -1.2 points versus placebo, favoring solriamfetol.
Clinician and patient global ratings also favored treatment.
The odds ratio was 3.7 for clinician-rated improvement and 4.2 for patient-rated improvement.
That convergence makes the trial more persuasive than a single lab measure would be.
Solriamfetol was not free of side effects, but the overall adverse-event rate was not higher than placebo in this small trial. Headache and nausea were the most common events.
Why Early Shift Disorder Is Clinically Awkward
The obvious non-drug answer is better scheduling. Later start times, protected sleep opportunity, light management, and consistent routines all matter. But many workers do not control the clock that governs their job.
That creates a clinical dilemma.
A medication can improve alertness, but it does not fix the underlying mismatch between circadian biology and work demands.
It may also carry cost, access, and long-term safety tests that a four-week trial cannot settle.
Still, the trial gives clinicians more direct evidence for a population that is easy to overlook.
Early-morning shift workers are not just “morning people having a hard week.” Some meet criteria for shift work disorder and have persistent excessive sleepiness that affects functioning and safety.
A Four-Week Trial Leaves Long-Term tests
The study was randomized and blinded, which is a strength.
But it was also small and short.
It cannot tell us what happens after months or years of use, whether benefits persist, whether tolerance emerges, or how the drug interacts with real-world sleep extension strategies.
The funding, including Axsome Therapeutics, also deserves ordinary scrutiny. Industry-funded trials can be rigorous, but replication and postmarketing data still matter.
The practical takeaway is focused: solriamfetol showed clear short-term efficacy for excessive sleepiness in early-morning shift work disorder.
That is not a license to ignore sleep timing, but it is a serious readout for a problem hiding in millions of alarm clocks.
How Solriamfetol Differs From Simply Adding Caffeine
Many early-shift workers already self-medicate with caffeine.
The difference is that solriamfetol was tested as a structured pharmacologic intervention with objective wakefulness and clinical global ratings as outcomes.
It acts through dopamine and norepinephrine reuptake inhibition rather than through adenosine receptor blockade.
That does not automatically make it better for every person. Caffeine is cheap, familiar, and short-acting for many users.
Solriamfetol is a prescription medication with its own adverse-effect profile and clinical screening needs. But the trial gives physicians evidence beyond the usual advice to sleep more and drink coffee earlier.
The most relevant patient is not a sleepy person after one bad night. It is someone with recurrent excessive sleepiness tied to a work schedule that repeatedly collides with circadian biology.
Alertness Medication Cannot Fix a Broken Schedule
The trial should not become a workplace excuse to preserve punishing schedules.
A medication that improves wakefulness can reduce symptoms, but it does not give workers more sleep opportunity, restore family timing, or remove the metabolic and cardiovascular stressors associated with circadian disruption.
The distinction is important ethically.
Pharmacology can help individuals who cannot change their shifts.
It should not become the only intervention society offers people whose jobs require them to wake when the brain is designed to sleep.
For occupational health, that means medication evidence should sit beside scheduling evidence.
If a workplace can adjust start times, protect sleep opportunity, or reduce safety-critical work during the circadian low point, those fixes still address the cause more directly.
The individual patient may still need help while those larger fixes are unavailable.
That is the narrow space where this trial is most helpful: not as a substitute for healthier schedules, but as evidence for symptom relief when schedule control is limited.
That narrowness is a strength because it keeps a helpful medication readout from becoming a workplace policy shortcut.
A Wakefulness Test Captured More Than Feeling Tired
The Maintenance of Wakefulness Test is helpful because subjective sleepiness can be noisy.
Some workers underreport impairment because they are used to functioning while tired; others may feel terrible while still performing adequately on objective measures.
By using sleep latency as the primary endpoint, the trial measured physiological ability to remain awake.
That is especially relevant when the consequences of sleepiness are not just discomfort but driving risk, workplace accidents, and impaired decision-making.
The trial also gives future studies a practical benchmark for sleep clinicians.
If a larger, longer study cannot reproduce an objective wakefulness gain in this range, the clinical case becomes weaker; if it can, early-morning shift disorder starts looking like a much more treatable circadian-sleepiness phenotype.
Citation: DOI: 10.1056/EVIDoa2500190. Zitting et al. Solriamfetol for Excessive Sleepiness in Early-Morning Shift Work Disorder. NEJM Evidence. 2026
Study Design: Randomized, double-blind, placebo-controlled clinical trial.
Sample/Model: 78 early-morning shift workers with excessive sleepiness associated with shift work disorder.
Key Statistic: Solriamfetol improved Maintenance of Wakefulness Test sleep latency by 9.4 minutes versus placebo after 4 weeks (95% CI, 5.7 to 13.0; P<0.001).
Caveat: Single-study evidence; interpret with the source design and sample.