TL;DR: A 2026 review in CNS Drugs argues that seletracetam, an unapproved SV2A-targeting antiseizure drug, may deserve renewed development as a low-volume intranasal non-benzodiazepine rescue treatment for acute repetitive seizures.
Key Findings
- SV2A racetam: Seletracetam is a second-generation racetam related to levetiracetam and brivaracetam.
- Phase IIa history: Oral seletracetam reached early clinical trials but was discontinued as oral epilepsy therapy while brivaracetam advanced.
- >90% bioavailability: Phase I studies reported rapid and extensive oral absorption, linear pharmacokinetics, and an approximately 8-hour half-life.
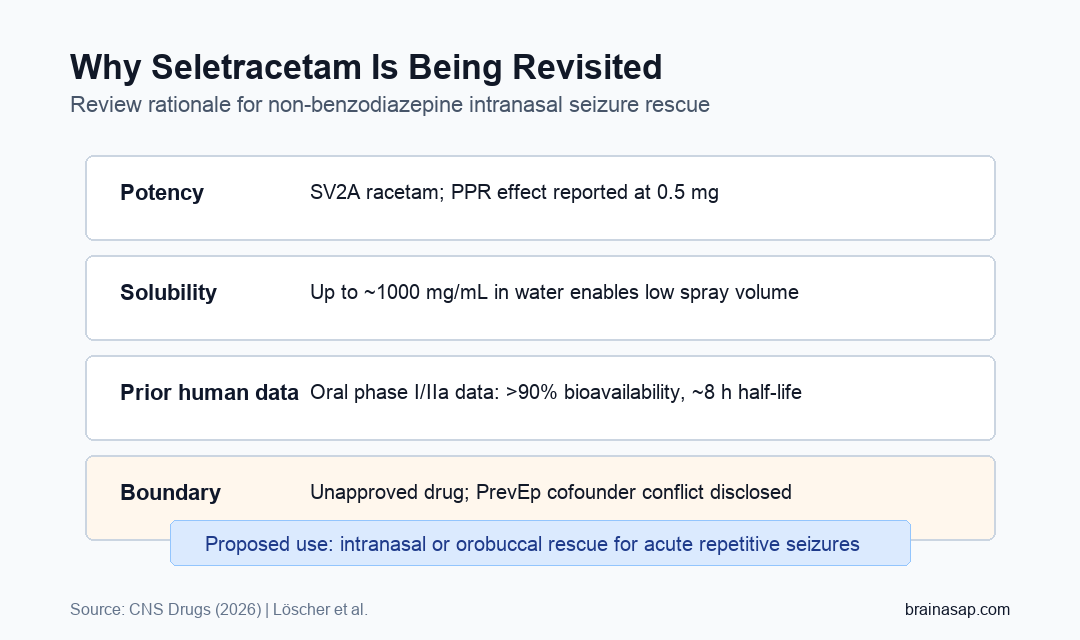
- 0.5 mg PPR effect: In photosensitive epilepsy, photoparoxysmal-response suppression was reported at doses as low as 0.5 mg.
- 2024-2025 patent activity: PrevEp filed new intranasal and orobuccal seletracetam formulation patent applications for seizure rescue use.
Source: CNS Drugs (2026) | Löscher et al.
Seletracetam is not a new approved epilepsy medicine. It is an older drug candidate that reached early human testing, lost development momentum, and is now being reconsidered for a different purpose.
The review’s central argument is pharmacological: seletracetam’s potency and water solubility could make it suitable for a low-volume intranasal rescue spray, a use case where many antiseizure drugs are impractical.
Seletracetam Targets SV2A Like Levetiracetam and Brivaracetam
Seletracetam belongs to the racetam antiseizure-drug family. Like levetiracetam and brivaracetam, it acts through synaptic vesicle glycoprotein 2A (SV2A), a protein involved in synaptic neurotransmitter release.
The original discovery program screened about 12,000 compounds for binding to the levetiracetam binding site, later characterized as SV2A. Around 1,200 compounds then moved into animal seizure-protection screening.
- Levetiracetam: Established SV2A-targeting antiseizure medication.
- Brivaracetam: Higher-potency SV2A racetam that advanced to phase III trials and FDA approval for focal-onset seizures.
- Seletracetam: Highly potent SV2A racetam that stayed behind as a backup after oral development was discontinued.
The review states that seletracetam had at least 10 times higher SV2A affinity than levetiracetam and strong potency in several animal models, especially the amygdala kindling model.
That animal-model potency is one reason the route question became important. A drug can have strong antiseizure activity and still be hard to use for rescue treatment if the required dose cannot fit into a fast, tolerable delivery format.
Oral Seletracetam Had Phase I and Phase IIa Human Data
The human evidence summarized in the review comes mainly from oral seletracetam studies. Phase I studies reported >90% bioavailability, linear pharmacokinetics, and an elimination half-life of about 8 hours.
Clinical adverse events were described as mostly mild to moderate central nervous system effects. The review also states that oral seletracetam did not show the respiratory-depression or addictive-potential profile associated with benzodiazepine rescue drugs.
- Photosensitive epilepsy: Phase IIa studies found suppression of photoparoxysmal responses.
- Drug-resistant focal epilepsy: Early trials reported efficacy and a favorable safety profile.
- Development stop: Oral development ended while brivaracetam continued into larger trials.
Intranasal Seizure Rescue Is the New Development Rationale
Current acute seizure rescue therapy often relies on benzodiazepines, including intranasal, buccal, rectal, or injectable formulations. They can stop seizures, but sedation and respiratory-risk concerns remain clinically important.
Seletracetam’s potential advantage is formulation. The review states that up to about 1000 mg/mL can dissolve in water, allowing therapeutic doses in very low liquid volumes.
This property is relevant for intranasal delivery because the nose can only accept a limited spray volume comfortably. A highly soluble and potent non-benzodiazepine drug is easier to package into a small rescue dose.
Rescue treatment also has a different job than daily antiseizure therapy. It needs rapid absorption, a practical route for caregivers, and enough tolerability that treatment can be used during urgent seizure clusters without adding avoidable respiratory risk.
- High potency: Less drug may be needed to reach an active dose.
- Water solubility: The drug can be formulated in a concentrated liquid.
- Non-benzodiazepine mechanism: SV2A modulation differs from GABAergic benzodiazepine action.
Patent Filings Reopened Seletracetam for Rescue Use
Seletracetam’s original patent expired in 2021. The review notes that PrevEp filed a US patent application in 2024 and a worldwide Patent Cooperation Treaty application in 2025 for intranasal and orobuccal seletracetam formulations and medical uses.
The drug is not approved or ready for routine rescue use. Development has restarted around a new formulation and indication.
The review also mentions first-in-human intranasal spray experience, but broad clinical claims still require controlled trials that directly test seizure rescue outcomes, onset, safety, and usability outside the clinic.
Those trials would need to answer practical questions: how fast seizures stop, how often seizures recur, whether repeat dosing is needed, and whether caregivers can administer the spray correctly during an emergency.
Conflict and Approval Status Keep the Claim Bounded
The review is scientifically detailed, but its conflict context should be visible. The conflict disclosure states that the authors are cofounders of PrevEp, the company pursuing the new seletracetam rescue formulation.
That disclosure does not invalidate the pharmacology, but it raises the need for independent replication and controlled clinical testing. Seletracetam has also never been approved for human use, so it remains a new chemical entity in regulatory terms.
- Supported claim: Prior oral data and physicochemical properties support seletracetam as a plausible rescue-therapy candidate.
- Unsupported claim: The review does not prove that intranasal seletracetam is clinically superior to approved benzodiazepine rescue treatments.
- Required next step: Controlled rescue-use trials must test seizure termination, recurrence, sedation, respiratory safety, and caregiver usability.
The clinical claim remains conditional: a potent SV2A drug with high water solubility could fill a non-benzodiazepine rescue-treatment niche if future trials confirm real-world seizure-rescue performance.
Citation: DOI: 10.1007/s40263-026-01281-0. Löscher et al. Seletracetam revisited: A missed opportunity for effective epilepsy therapy. CNS Drugs. 2026;40:603-622.
Study Design: Narrative pharmacology and clinical-development review of seletracetam.
Sample/Model: Preclinical epilepsy models plus prior phase I and phase IIa oral seletracetam human studies.
Key Statistic: Phase I oral data reported >90% bioavailability and an approximately 8-hour elimination half-life; PPR suppression was reported at 0.5 mg in photosensitive epilepsy.
Caveat: Seletracetam is not approved, and the review authors disclosed PrevEp cofounder conflicts related to the new rescue formulation.