TL;DR: A 2026 preprint in medRxiv reported that one session of left central thalamus focused ultrasound increased behavioral responsiveness scores in 16 adults with chronic disorders of consciousness, with no severe adverse events reported.
Key Findings
- 16 chronic DOC patients: Adults had chronic disorders of consciousness after severe brain injury, with an average time since injury of 3.39 years.
- Single thalamic target: Low-intensity transcranial focused ultrasound was delivered once to the left central thalamus during a 10-day inpatient protocol.
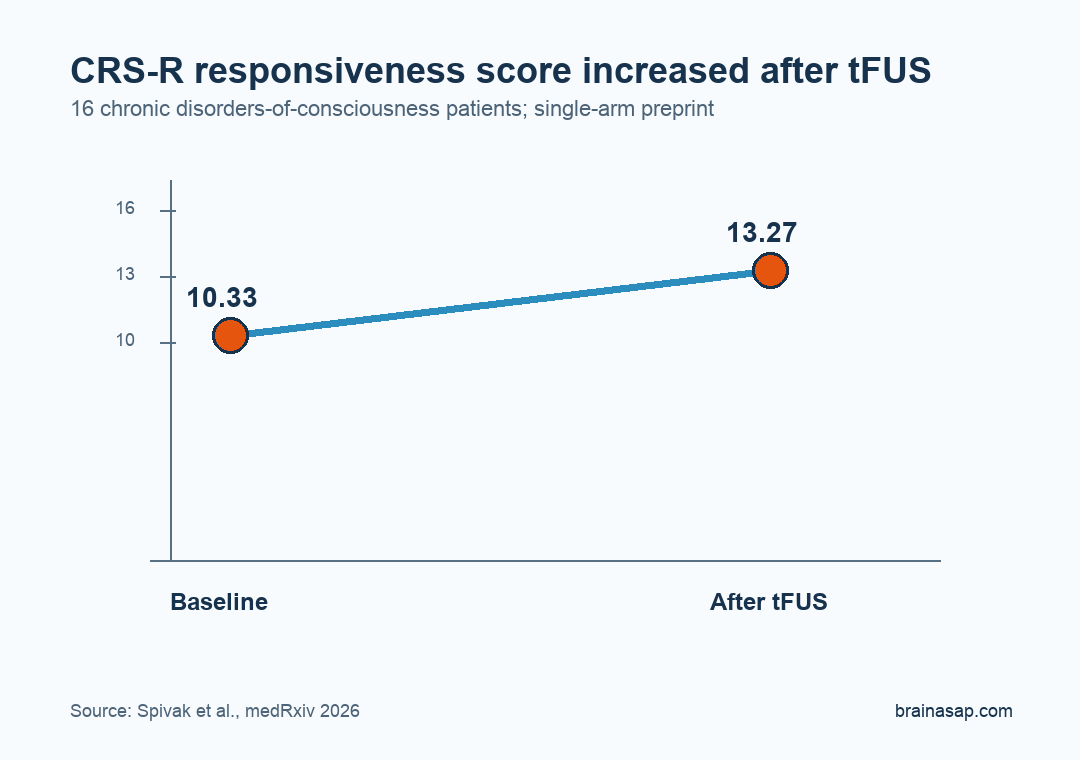
- CRS-R score increased: Maximum Coma Recovery Scale-Revised scores increased from 10.33 at baseline to 13.27 after sonication.
- Electroencephalography (EEG) slowing predicted gains: The global delta/beta ratio increased, and frontal slowing predicted behavioral improvement with Kendall tau-b = 0.51.
- No severe adverse events: Researchers reported no severe adverse events, supporting a larger sham-controlled trial rather than immediate clinical adoption.
Source: medRxiv (2026) | Spivak et al.
Transcranial focused ultrasound (tFUS) is being studied as a noninvasive way to modulate deep brain structures. In this trial, researchers aimed ultrasound at the thalamus, a relay region involved in arousal, sleep-wake regulation, and large-scale brain communication.
The patients had chronic disorders of consciousness (DOC), meaning persistent impaired awareness after severe brain injury. The study tested whether a single sonication could shift behavior, electroencephalography, metabolism, and sleep measures in the same direction.
Focused Ultrasound Targeted the Left Central Thalamus
The study used a single-arm open-label design, so every participant received the active intervention and there was no sham-control group. That design can show feasibility and within-person change, but it cannot fully separate treatment effects from natural fluctuation, measurement timing, or inpatient observation.
Participants were assessed during a 10-day inpatient protocol. The sample included 16 adults, 44% female, with a mean age of 37.81 years. Injury causes were mixed: 44% traumatic brain injury and 56% non-traumatic severe brain injury.
- Target: Left central thalamus, chosen because thalamocortical circuits are closely tied to arousal and responsiveness.
- Intervention: One session of low-intensity tFUS rather than implanted deep brain stimulation.
- Population: Chronic DOC patients, not acute coma patients, with an average 3.39 years since injury.
The chronic timing is important. A behavioral increase years after injury is harder to attribute to ordinary early recovery than a change seen soon after trauma, but the lack of a sham arm still keeps the causal claim bounded.
The outcome battery was deliberately broad. Instead of relying only on bedside behavior, the protocol paired clinical scoring with brain electrical activity, glucose-metabolism imaging, and sleep staging, giving the study several ways to look for a converging physiological response.
Coma Recovery Scores Increased After Sonication
The main behavioral outcome was the Coma Recovery Scale-Revised (CRS-R), a structured exam used to assess auditory, visual, motor, verbal, communication, and arousal responses in DOC. Higher CRS-R scores reflect more observable responsiveness.
Maximum CRS-R total score increased from 10.33 at baseline to 13.27 after tFUS. The reported test statistic was t(14) = 7.407, p < 0.001, with a large effect size, d = 1.913.
That score shift is clinically meaningful enough to justify further testing, but the single-arm design limits the interpretation. DOC exams can vary across days, and the strongest future test is a randomized sham-controlled trial with blinded raters.
EEG, FDG-PET, and Sleep Measures Pointed to a Thalamocortical Shift
Behavior was not the only measurement. Researchers also used electroencephalography (EEG), fluorodeoxyglucose positron emission tomography (FDG-PET), and polysomnography, a sleep-recording method.
The EEG analysis focused on the delta/beta ratio. Delta activity is slower electrical activity, beta activity is faster activity, and the ratio can describe broad arousal-state changes.
The global delta/beta ratio increased after sonication. Frontal slowing also predicted behavioral gains, suggesting that the most responsive patients may have had a measurable electrophysiological state shift.
- EEG outcome: The global delta/beta ratio increased in 14 analyzed participants, with W = 17, p = 0.025, and r = 0.68.
- Prediction signal: Frontal slowing predicted CRS-R improvement with tau-b = 0.51 and p = 0.016.
- FDG-PET outcome: Glucose metabolism decreased bilaterally in the thalamus and in frontal, temporal, and parietal cortices at post-tFUS timepoints.
- Sleep outcome: N2 sleep increased by 33% in 11 participants, although that result did not survive correction.
These measures support the proposed thalamocortical reset mechanism. The word “reset” should be read as a mechanistic hypothesis, not proof that ultrasound restored consciousness through one defined pathway.
No Severe Adverse Events Were Reported, but the Trial Was Small
Safety was a necessary part of the study because focused ultrasound can alter neural activity without surgery. The preprint reported no severe adverse events during the protocol.
That safety result is encouraging but early. Sixteen patients cannot detect rare adverse effects, and a single-session inpatient protocol does not answer whether repeated sonication would remain tolerable.
The disclosure context also deserves attention. One investigator reported consulting for BrainSonix Corp, the device manufacturer, which makes independent replication and blinded outcome assessment especially important for the next trial.
- No sham control: The design cannot rule out expectancy, measurement variability, or natural day-to-day changes in responsiveness.
- Small sample: The study had 16 participants, with fewer participants in some EEG and sleep analyses.
- Mixed injuries: Traumatic and non-traumatic injury mechanisms may not respond to thalamic modulation in the same way.
- Device conflict: One investigator disclosed consulting for the ultrasound-device manufacturer, so independent replication is especially important.
The preprint is strongest as a mechanistic clinical-trial signal. It supports a larger randomized sham-controlled study that can test whether thalamic tFUS reliably improves DOC outcomes and which physiological marker best predicts response.
Citation: DOI: 10.64898/2026.05.26.26354167. Spivak et al. Thalamic sonication in chronic disorders of consciousness: a mechanistic single-arm clinical trial. medRxiv. 2026.
Study Design: Single-arm, open-label, inpatient mechanistic clinical trial of one tFUS session.
Sample Size: 16 adults with chronic disorders of consciousness after severe brain injury.
Key Statistic: Maximum CRS-R total score increased from 10.33 to 13.27 after sonication; t(14) = 7.407, p < 0.001.
Caveat: The study was small, open-label, and not sham-controlled, so efficacy needs randomized blinded testing.