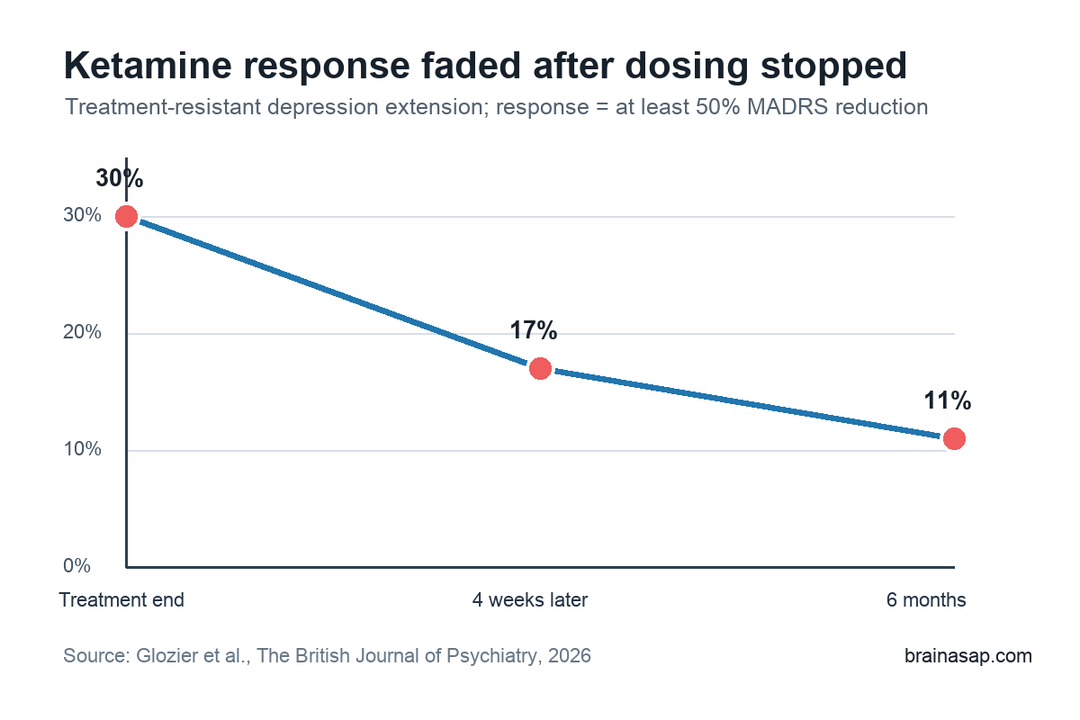
TL;DR: A 2026 study in The British Journal of Psychiatry found that 4 weeks of twice-weekly subcutaneous racemic ketamine helped a minority of people with treatment-resistant depression, but response fell from 30% at treatment end to 17% 4 weeks later.
Key Findings
- 130 trial participants entered the extension: All had treatment-resistant depression and a Montgomery-Asberg Depression Rating Scale (MADRS) score of 20 or higher after the prior randomized trial.
- Ketamine was given twice weekly for 4 weeks: Participants received subcutaneous racemic ketamine, either at 0.5 mg/kg or in a flexible 0.5-0.9 mg/kg response-guided regimen.
- 30% met response criteria at treatment end: Response meant at least a 50% reduction in MADRS depression severity from open-label extension baseline.
- Response faded after dosing stopped: 4 weeks later, 17% still met response criteria; by 6 months, 11% did.
- No unexpected safety pattern emerged: Researchers reported expected transient effects, no suicide or self-harm events requiring admission, and no clear cumulative safety problem through 6 months.
Subcutaneous racemic ketamine produced uneven short-term outcomes in people whose depression had already resisted treatment. The open-label extension followed participants from the Ketamine for Adult Depression Study, giving all eligible participants 4 more weeks of ketamine and then tracking outcomes after dosing ended.
The clinical pattern was selective rather than broadly durable: some participants improved substantially, while most did not reach the study’s response threshold and many gains weakened after treatment stopped.
4 Weeks of Ketamine Lowered MADRS Scores
Researchers enrolled 130 adults from the earlier randomized trial. To enter the extension, participants had to have a post-trial MADRS score of at least 20, meaning they still had clinically important depressive symptoms after the first trial phase.
The extension used 2 dosing approaches:
- Fixed regimen: 0.5 mg/kg subcutaneous racemic ketamine twice weekly for 4 weeks.
- Flexible regimen: 0.5-0.9 mg/kg twice weekly, with dose increases guided by response.
The combined group improved by an average of 8.6 MADRS points, moving from a baseline mean of 28.8 to 20.3 at the end of the 4-week extension. The average reduction was clinically visible, but individual response varied widely.
At treatment end, 35 of 116 assessed participants met the study’s response definition: at least a 50% drop in MADRS score. That worked out to 30%.
Remission was less common, depending on the cutoff used: 18% had a MADRS score of 10 or lower, and 26% had a score of 12 or lower.
Most Participants Did Not Have a Large Response
The same table also shows why the result should not be oversold. More than half of the assessed participants had a less than 25% MADRS reduction at each major time point.
At treatment end, the response profile was:
- 30% responded: MADRS score fell by at least 50%.
- 26% met the broader remission cutoff: MADRS score was 12 or lower.
- 51% were nonresponders: MADRS score fell by less than 25%.
The split is clinically important. Subcutaneous ketamine may be worth considering for some people with treatment-resistant depression, but the extension does not support a simple expectation that most patients will respond strongly after 4 weeks.
Clinician ratings were somewhat more favorable than the strict MADRS response threshold. By the end of treatment, 45% were rated as “very much” or “much” improved, and the share rated as having mild illness or better increased from 8% at extension baseline to 46%.
The Response Faded After Treatment Stopped
The follow-up pattern is the central caution. At 4 weeks after dosing stopped, only 19 of 110 assessed participants still met response criteria, or 17%.
At 6 months, the response rate was 8 of 73, or 11%.
Mean symptoms also drifted back upward. The mean MADRS score was 20.3 at treatment end, then 22.6 4 weeks later and 24.8 at 6 months.
Scores remained below the extension baseline, but the strongest improvement was not sustained for many participants.
This is consistent with the broader ketamine literature: rapid improvement can happen, but maintaining that improvement is a separate treatment question.
Flexible Dosing Did Not Clearly Beat Fixed Dosing
The trial changed dosing after a Data Safety Monitoring Board recommendation, creating a smaller fixed-dose group and a larger flexible-dose group. In the extension, 32 participants received the fixed regimen and 98 received flexible dosing.
Researchers did not find consistent response differences between those 2 regimens. Both groups improved during treatment, and symptoms increased after treatment cessation.
The flexible schedule allowed higher doses, but this extension did not show a clear clinical advantage for flexible dosing over 0.5 mg/kg.
Prior ketamine exposure also had a limited association with retreatment. Participants who had received ketamine during the randomized trial showed a smaller response after the first extension treatment, but that difference did not persist across later assessments.
Prior response was more informative than prior exposure:
- Prior responders often responded again: 9 of 11 earlier ketamine responders who relapsed after the randomized trial responded again in the extension.
- Prior nonresponse was not final: About 25% of prior ketamine nonresponders responded during retreatment.
- Placebo nonresponders also sometimes responded: 13 of 58 prior midazolam nonresponders responded once they received ketamine in the extension.
No Unexpected Safety Pattern Was Seen
Safety findings were reassuring but still bounded by the study design. 3 severe adverse events occurred in the flexible-dose group, and researchers judged them unrelated to ketamine treatment.
Expected acute effects included transient blood-pressure changes and short-term dissociative or treatment-emergent symptoms. Researchers reported no suicide or self-harm events requiring admission during treatment or within 2 months after cessation, and no observed cumulative adverse pattern through 6 months.
The evidence still has limits:
- Open-label design: Everyone knew ketamine was being given, so expectancy and care effects cannot be separated cleanly.
- Attrition after treatment: Follow-up numbers fell by 6 months, which makes later response estimates less certain.
- Highly resistant sample: Results may not generalize to people with less severe or less chronic depression.
This extension supports subcutaneous ketamine as a potentially useful short-term option for a subset of people with treatment-resistant depression. It also shows why clinicians and patients need a maintenance plan, because the average benefit weakened once the 4-week dosing course ended.
Citation: DOI: 10.1192/bjp.2026.10692. Glozier et al. Effectiveness and safety of repeat dose subcutaneous ketamine for treatment-resistant depression, and the impact of prior ketamine treatment: open label extension of the KADS study. The British Journal of Psychiatry. 2026.
Study Design: Open-label extension of a randomized controlled trial at seven mood disorder centers in Australasia.
Sample Size: 130 adults with treatment-resistant depression entered the extension; 116 were assessed at treatment end.
Key Statistic: Response fell from 30% at treatment end to 17% 4 weeks later and 11% at 6 months.
Caveat: The extension was open label and follow-up attrition makes later response rates less certain.