TL;DR: A 2026 systematic review and meta-analysis in Pain Medicine found that Medicaid enrollment and preoperative benzodiazepine use had the largest pooled associations with new persistent opioid use after surgery among opioid-naive US adults.
Key Findings
- 27 cohort studies: The review included US adult surgical studies that separated opioid-naive patients from those using opioids before surgery.
- 6093 records screened: Database searching led to 3121 title/abstract screens and 152 full-text reviews.
- 1.77 Medicaid OR: Medicaid enrollment had a pooled odds ratio of 1.77 for new persistent opioid use.
- 1.77 benzodiazepine OR: Preoperative benzodiazepine use had the same pooled odds ratio, 1.77.
- 1.24 mood-disorder OR: Mood disorders and anxiety were also associated with higher odds, with pooled odds ratios of 1.24 and 1.17.
Source: Pain Medicine (2026) | Lee et al.
New persistent opioid use means continued opioid use beyond the expected surgical recovery window in someone who was opioid-naive before surgery. In this review, the threshold was opioid use at least 3 months after surgery.
The distinction matters because a patient already using opioids before surgery has a different risk profile than a patient whose first prolonged exposure begins with postoperative pain treatment.
The Review Focused on Opioid-Naive US Surgical Patients
Researchers reviewed recent US evidence on patient-related risk factors for new persistent opioid use after surgery. The protocol was registered in PROSPERO, and the review followed PRISMA reporting standards.
The search identified 6093 records. After duplicate removal, researchers screened 3121 studies by title and abstract, reviewed 152 full texts, and included 27 retrospective cohort studies.
- Population: Adults in the United States who were opioid-naive before surgery.
- Outcome: Opioid use continuing at least 3 months after surgery.
- Evidence base: All included studies were retrospective cohort studies.
- Quality rating: 24 studies were rated good quality and 3 were rated fair quality.
Included surgeries ranged across cardiothoracic, orthopedic, gynecologic, endocrine, gastrointestinal, and urologic procedures. Sample sizes varied widely, from 248 to 2,957,115 participants.
Medicaid and Benzodiazepine Use Had the Largest Pooled Associations
The meta-analysis focused on risk factors that were measured comparably across studies. Four factors met that bar: mood disorders, anxiety, Medicaid enrollment, and preoperative benzodiazepine use.
Medicaid enrollment and preoperative benzodiazepine use had the largest pooled estimates. Each had a pooled odds ratio of 1.77.
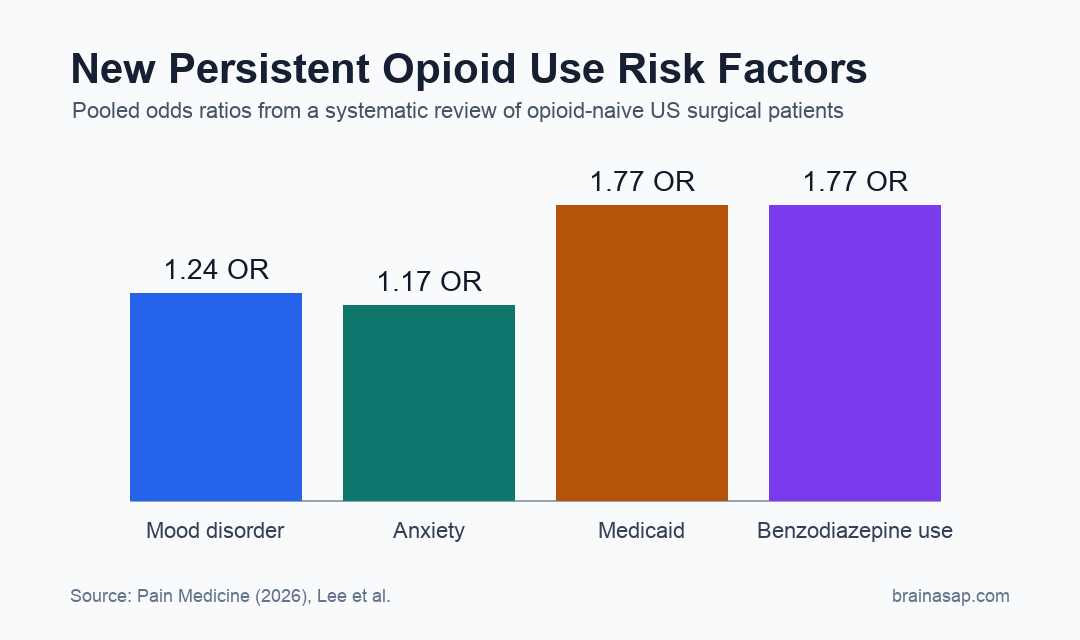
- Mood disorders: 17 studies produced a pooled odds ratio of 1.24.
- Anxiety: 13 studies produced a pooled odds ratio of 1.17.
- Medicaid enrollment: 4 studies produced a pooled odds ratio of 1.77.
- Benzodiazepine use: 6 studies produced a pooled odds ratio of 1.77.
The Medicaid estimate likely reflects more than insurance paperwork. The authors discussed links with socioeconomic vulnerability, health care access, and prescribing patterns, but the review could not isolate which pathway drove the association.
Mood Disorders and Anxiety Added Smaller but Consistent Risk
Mood disorders and anxiety had smaller pooled estimates than Medicaid enrollment or benzodiazepine use, but the direction was consistent. Mood disorders were associated with 24% higher odds, and anxiety with 17% higher odds.
Those associations are clinically plausible because mood and anxiety disorders can overlap with higher pain sensitivity, more severe postsurgical pain, and higher general opioid exposure. They can also complicate recovery expectations and follow-up care.
- Preoperative screening: Mood disorders and anxiety can be identified before surgery.
- Care planning: Patients with higher risk may need clearer pain plans and closer postoperative monitoring.
- Medication review: Benzodiazepines deserve explicit review because concurrent opioid-benzodiazepine exposure raises safety concerns.
The review does not imply that these risk factors are interchangeable. Insurance status, psychiatric diagnoses, medication exposure, surgical pain, and access to follow-up can interact in the same patient.
Opioid Exposure Measures Also Pointed to Prescribing Decisions
Beyond the pooled meta-analysis, the narrative synthesis found that opioid exposure patterns also mattered. Filling opioid prescriptions before surgery, larger discharge amounts, and longer days supplied were each linked to higher risk in the included studies.
One cited pattern was a dose relationship. Initial opioid prescriptions greater than 300 morphine milligram equivalents were associated with higher odds of new persistent use in multiple studies.
- Prescription timing: Preoperative fills were associated with higher risk than postoperative-only fills in several studies.
- Prescription amount: Larger initial opioid quantities were linked to higher new persistent use risk.
- Days supplied: More than 7 days and especially more than 26 days of postoperative supply were associated with higher risk in one included study.
These prescribing variables are not purely patient-related, so they were handled differently from mood, anxiety, Medicaid, and benzodiazepine status. They still point to modifiable clinical workflows.
Claims-Based Evidence Cannot Confirm Opioid Consumption
The review’s main limitation is measurement. Most included studies used insurance claims or prescription records, which show fills or dispensing rather than confirmed pill consumption.
That means some patients may have filled opioids but not taken them, while others may have used non-prescribed opioids or paid cash outside the available data. Uninsured patients were also not well represented.
Claims data still have value for this question because they capture large surgical populations and objective prescribing records. They are strongest for identifying risk patterns that deserve prospective follow-up.
The pooled estimates also had substantial heterogeneity, so the exact odds ratios should be treated as broad risk markers rather than precise patient-level prediction tools. The clinical message is narrower: preoperative mental health, benzodiazepine use, insurance-linked vulnerability, and opioid exposure deserve proactive review before and after surgery.
Citation: DOI: 10.1093/pm/pnaf182. Lee et al. Patient-related risk factors for new persistent opioid use after surgery among opioid-naive individuals in the United States: a systematic review and meta-analysis. Pain Medicine. 2026.
Study Design: Systematic review and random-effects meta-analysis of retrospective cohort studies.
Sample Size: 27 included cohort studies; individual study sizes ranged from 248 to 2,957,115 participants.
Key Statistic: Medicaid enrollment and preoperative benzodiazepine use each had pooled odds ratios of 1.77 for new persistent opioid use.
Caveat: Most evidence came from claims or prescribing records, so opioid fills were not the same as verified consumption.