TL;DR: A 2026 medRxiv preprint linked greater attention-deficit/hyperactivity disorder (ADHD) symptom scores in college students to reduced stop-signal functional MRI (fMRI) activation in cannabinoid receptor 1 (CB1R)-rich brain regions, and that reduced activation predicted heavier cannabis-use trajectories over 4 years.
Key Findings
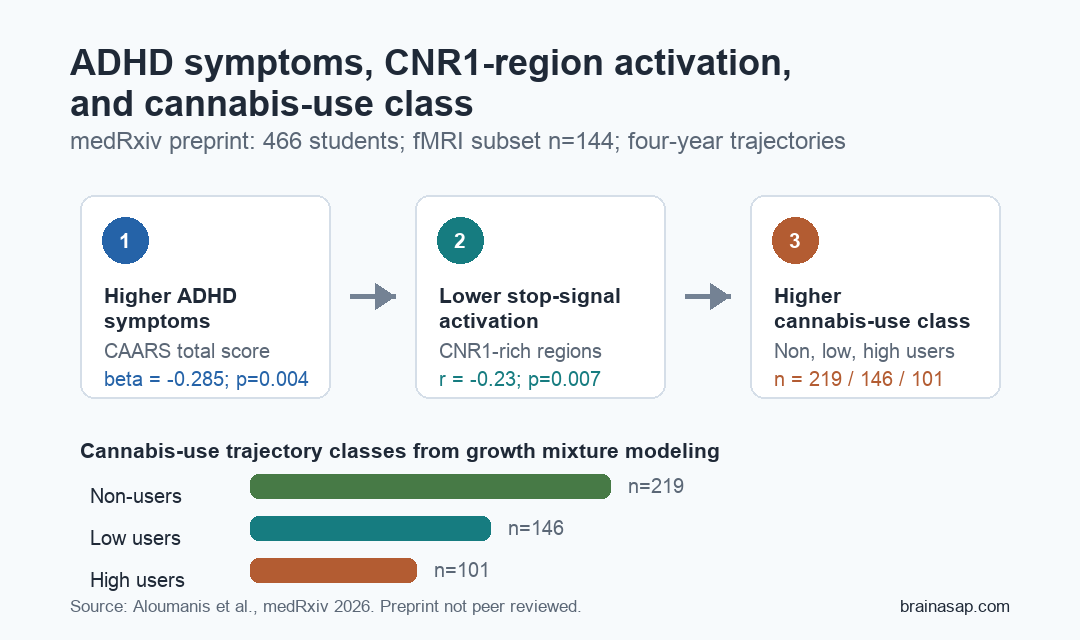
- ADHD-cannabis trajectory: Researchers analyzed cannabis-use trajectories in 466 first-year college students aged 18-19, with baseline ADHD symptom ratings and 3 yearly follow-up questionnaires.
- 144 functional MRI scans used: A neuroimaging subset completed a stop-signal task, an inhibitory-control test, while researchers measured brain activation during successful stopping.
- Three cannabis-use classes: Growth mixture modeling separated participants into non-users (n=219), low users (n=146), and high users (n=101).
- CNR1-region activation was reduced: Greater ADHD symptom severity predicted reduced stop-signal activation in CNR1-expressing regions (beta=-0.285, p=0.004).
- Higher-use class was predicted: Lower activation in CNR1-rich regions predicted higher cannabis-use class membership (beta=-0.139, p=0.028), while the indirect effect was only a trend (p=0.083).
Source: medRxiv (2026) | Aloumanis et al.
ADHD symptoms and cannabis use are often discussed as a behavioral overlap: impulsivity, attention problems, perceived self-medication, and higher risk for cannabis misuse.
This preprint tested a more specific biological question: whether ADHD symptom severity lined up with reduced activation in brain regions where the cannabinoid receptor 1 gene, CNR1, is more strongly expressed.
466 College Students Were Grouped by Cannabis-Use Trajectory
Researchers studied 466 first-year college students who were 18 or 19 years old at enrollment. Cannabis use was measured at baseline and during 3 yearly follow-ups, giving the analysis a longitudinal view rather than a single current-use snapshot.
ADHD symptom severity came from the Conners Adult ADHD Rating Scales (CAARS), a self-report questionnaire. ADHD diagnosis itself was not required for enrollment, so the analysis treated ADHD as a symptom continuum rather than a case-control comparison.
- Non-users: 219 participants reported no lifetime cannabis use at baseline and no cannabis use at any follow-up.
- Low users: 146 participants showed a lower-use trajectory across the follow-up period.
- High users: 101 participants showed a higher-use trajectory, with much higher average yearly use counts than the low-use group.
Average CAARS total ADHD symptom scores rose across those groups: 14.1 in non-users, 15.0 in low users, and 18.8 in high users. The group gradient does not prove ADHD symptoms caused cannabis use, but it set up the mediation test.
Stop-Signal Functional MRI Measured Inhibitory-Control Activation
A subset of 144 participants contributed usable functional MRI data during a stop-signal task. In this task, participants usually press a button in response to directional arrows, but on 25% of trials they receive a stop cue and must withhold the response.
The task is relevant because ADHD symptoms often involve difficulty with response inhibition, attention allocation, and impulsive action. Researchers focused on the contrast between successful stop trials and correct go trials to isolate inhibitory-control activation.
- Baseline questionnaires: Participants reported ADHD symptoms, cannabis use, alcohol use, childhood adversity, and socioeconomic measures.
- Brain activation: Functional MRI captured activation during the stop-signal task in the neuroimaging subset.
- Gene-expression map: CNR1 expression from the Allen Human Brain Atlas was mapped into the same brain space.
- Covariance measure: Each participant received a score reflecting how strongly stop-signal activation overlapped with higher-CNR1 regions.
Across the functional MRI group, stop-signal activation overlapped significantly with CNR1 expression (t(143)=5.17, p<0.001). The CNR1-overlap score therefore became the neural mediator for the next analysis.
CNR1-Rich Brain Regions Showed Lower Activation With More ADHD Symptoms
CNR1 encodes CB1R, the main cannabinoid receptor targeted by THC in the brain. CB1 receptors are dense in regions involved in inhibition, reward, movement, attention, and cortical control, making them biologically relevant to both cannabis effects and ADHD-related regulation.
Greater ADHD symptom scores correlated with reduced stop-signal activation in CNR1-expressing regions (r=-0.23, p=0.007). A separate analysis of task-positive regions also found a negative relationship between CAARS total ADHD symptoms and average activation (r=-0.30, p<0.001).
Cannabis-use class showed a weaker but directionally consistent activation pattern. Compared with non-users, high users had significantly lower CNR1-region stop-signal activation (beta=0.040, SE=0.018, p=0.027), while low users trended toward higher activation than high users (p=0.062).
- ADHD symptom path: Higher symptom severity predicted lower CNR1-region stop-signal activation.
- Cannabis class path: Lower CNR1-region activation predicted membership in a higher cannabis-use class.
- Group contrast: High users showed lower activation than non-users in the CNR1-overlap measure.
Mediation Result Supported a Partial, Preliminary Pathway
The mediation model asked whether CNR1-region stop-signal activation statistically connected ADHD symptoms with cannabis-use class. The model controlled for sex, recent cannabis use, baseline alcohol use, childhood adversity, family income, and missing income status.
Greater ADHD symptoms predicted less activation in CNR1-rich regions (beta=-0.285, p=0.004). Less activation then predicted higher cannabis-use class membership (beta=-0.139, p=0.028).
The total effect of ADHD symptoms on cannabis-use class was significant (beta=0.108, p=0.026), while the direct effect after accounting for the mediator was not significant (beta=0.068, p=0.189).
The indirect effect through the CNR1-region activation measure was only a trend (beta=0.040, p=0.083), so the mediation claim should stay preliminary.
Researchers also tested the reverse direction: whether baseline cannabis use predicted the CNR1-region activation measure, which then predicted ADHD symptoms. That reverse model did not support the same pathway, although the activation-ADHD relationship remained present.
Self-Medication Interpretation Is Plausible but Not Proven
The preprint fits the self-medication hypothesis in a narrow way. Students with higher ADHD symptom scores showed lower engagement of CB1R-linked inhibitory-control regions, and that lower engagement was associated with heavier cannabis-use trajectories.
The data do not show that cannabis treated ADHD symptoms in this sample. The study measured symptom ratings, brain activation, and use trajectories; it did not randomize cannabis exposure or test whether cannabis improved attention, inhibition, grades, daily function, or clinical ADHD outcomes.
- Supported claim: ADHD symptom severity was linked to lower activation in CNR1-rich inhibitory-control regions.
- Behavioral link: Lower activation predicted higher cannabis-use class membership over follow-up.
- Unsupported clinical leap: The data do not show that cannabis is an effective or safe ADHD treatment.
- Preprint boundary: The manuscript has not been certified by peer review and should not guide clinical practice.
For prevention research, the useful clinical target is earlier identification of students whose inhibitory-control circuitry, ADHD symptoms, and cannabis-use escalation may converge. Any treatment implication would need trials that directly measure ADHD outcomes and cannabis-related harms.
Self-Report ADHD Scores and Small Imaging Sample Limit the Claim
Several limits keep the result narrow. ADHD symptoms were measured once at baseline with self-report CAARS scores, not repeated clinical interviews, parent or clinician ratings, or a confirmed ADHD diagnosis.
The imaging subset was also modest: 144 participants contributed functional MRI data, while the mediation model used 450 participants after excluding missing baseline questionnaire data. The gene-expression map came from normative postmortem donor brains, so it did not measure each participant’s own CB1 receptor density.
Latent cannabis-use classes capture broad trajectory patterns, but they do not fully represent THC potency, route of administration, cannabis product type, age at first use, or polysubstance exposure. Those details could change how cannabis use relates to inhibitory-control networks.
Citation: DOI: 10.64898/2026.06.24.26356461. Aloumanis et al. ADHD Symptoms and Cannabis Use: The Role of Cannabinoid Receptor 1 and Neural Response Inhibition. medRxiv. 2026.
Study Design: Longitudinal college-student cohort with self-report ADHD symptoms, cannabis-use trajectory modeling, functional MRI stop-signal task data, and CNR1 gene-expression map integration.
Sample Size: 466 students for cannabis-use trajectories, 450 participants in mediation models, and 144 participants with usable functional MRI data.
Key Statistic: Greater ADHD symptom severity predicted reduced stop-signal activation in CNR1-rich regions (beta=-0.285, p=0.004), and reduced activation predicted heavier cannabis-use class (beta=-0.139, p=0.028).
Caveat: This is a non-peer-reviewed preprint using baseline self-report ADHD scores and a modest fMRI subsample, so it does not prove cannabis treats ADHD or establish causality.