TL;DR: A 2026 systematic review and meta-analysis in Bipolar Disorders found that poor medication adherence in bipolar disorder was linked to substance use, psychotic features, lower insight, poorer functioning, and several markers of more severe illness, but most evidence was graded low or very low quality.
Key Findings
- 19 studies included: Researchers pooled observational studies that separated people with bipolar disorder into poor-adherence and good-adherence groups using clinical or biological adherence measures.
- Substance use stood out: Poor adherence was associated with any substance use disorder, cannabis use disorder, and alcohol use disorder.
- Severity markers clustered: Psychotic features, suicide-attempt history, more manic and mixed episodes, more hospitalizations, higher global severity, lower insight, and lower functioning all tracked with poor adherence.
- Medication class did not explain the pattern: Lithium, valproate, carbamazepine, antidepressant, antipsychotic, and polytherapy comparisons did not show clear adherence differences.
- Evidence quality was limited: Cannabis use disorder had moderate-quality evidence, while most other correlates were graded low or very low because of small effects, heterogeneity, imprecision, or publication-bias risk.
Source: Bipolar Disorders (2026) | Bartoli et al.
For clinicians, this is a triage signal. A missed-dose history may need to be read together with comorbidity, illness course, and practical support rather than as an isolated behavior.
The review pooled observational studies, so the safer reading is risk profiling rather than causal certainty. Poor adherence marks a higher-risk clinical profile that may need earlier and more structured support.
Researchers Pooled 19 Bipolar Disorder Adherence Studies
The analysis included 19 studies of adults with bipolar disorder. Study samples ranged from 44 to 2,205 people, and poor-adherence rates varied widely, from 13.9% to 69.3%.
Researchers limited inclusion to studies with clearer adherence definitions. Some used clinician evaluation, some used blood concentrations of psychotropic medications, and some combined clinical assessment with biological measures.
The measurement choice is important because adherence is hard to capture. Self-report alone can miss skipped doses, partial dosing, or treatment interruptions.
Clinical and blood-level measures are still imperfect, but they are closer to the behavior the review was trying to study.
- Search scope: MEDLINE, Embase, and PsycInfo were searched through March 2025.
- Evidence base: The final meta-analysis tested 38 sociodemographic, clinical, treatment, and functioning variables.
- Main comparison: Each variable was compared between people classified as poorly adherent and those classified as adherent.
Substance Use Had the Clearest Adherence Signal
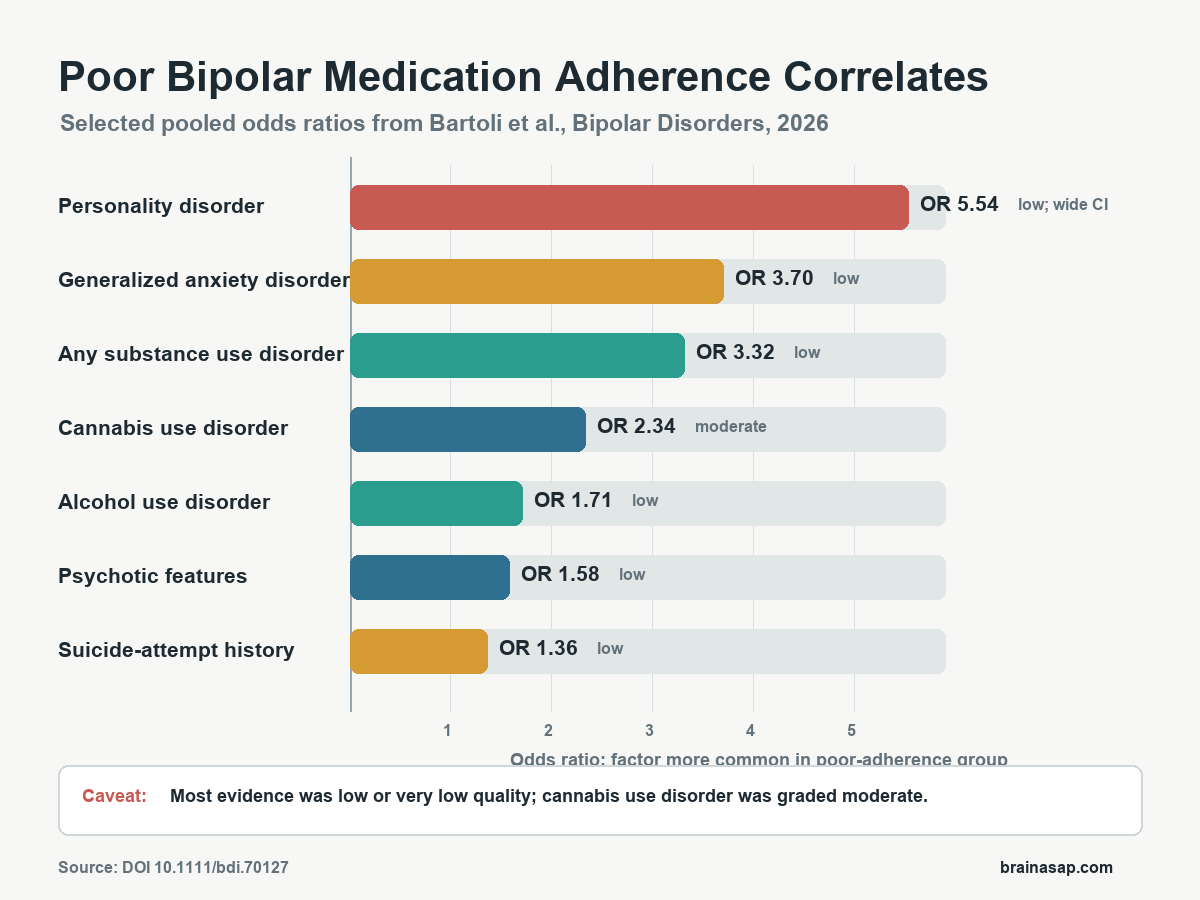
The strongest clinical cluster involved substance use. Poor adherence was associated with any substance use disorder, with a pooled odds ratio of 3.32.
Cannabis use disorder had an odds ratio of 2.34, and alcohol use disorder had an odds ratio of 1.71.
The cannabis result deserves special attention because it was the only correlate graded as moderate-quality evidence. Most other findings were downgraded because there were too few studies, inconsistent estimates, wide confidence intervals, small effects, or possible publication bias.
Clinically, the substance-use pattern is plausible. Alcohol or cannabis use can disrupt routines, increase mood instability, complicate medication side effects, and reduce confidence in maintenance treatment.
The analysis cannot prove which direction dominates, but it makes substance-use screening central to adherence work.
Psychotic Features and Suicide-Attempt History Also Tracked With Poor Adherence
Several illness-severity markers were associated with poor medication adherence. People in the poor-adherence groups were more likely to have psychotic features, with an odds ratio of 1.58, and a history of suicide attempts, with an odds ratio of 1.36.
Episode history also mattered. Poor adherence was linked to more previous manic episodes and more mixed episodes, while the number of previous depressive episodes did not show a clear difference.
The authors offered a clinical interpretation: manic and mixed states may reduce perceived need for treatment, impair judgment, or make medication routines harder to sustain. Depressive episodes may be more subjectively distressing, which can sometimes increase help-seeking and treatment engagement.
- Earlier onset: Poor-adherence groups had a younger age at bipolar disorder onset.
- Hospital burden: Poor adherence was linked to a higher number of previous hospitalizations.
- Comorbid anxiety: Generalized anxiety disorder showed a strong association, with an odds ratio of 3.70, though the evidence came from only three studies.
- Personality disorder: Comorbid personality disorder was also associated with poor adherence, but the confidence interval was wide.
Lower Insight and Functioning Were Part of the Same Pattern
Adherence was also tied to how well people understood and functioned with the illness. Poor-adherence groups had lower insight, with a standardized mean difference of -0.74, and lower global functioning, with a standardized mean difference of -0.60.
Those are not minor clinical details. A person who has limited insight into bipolar disorder, has trouble functioning day to day, and has co-occurring substance use may need more than a reminder to take medication.
The care plan may need practical supports, family involvement when appropriate, psychoeducation, side-effect management, and frequent early follow-up.
Lower education and not being in a relationship also tracked with poor adherence. Those findings point toward social and cognitive context, not just symptom severity.
People with fewer supports or less health-literacy reserve may have more trouble maintaining a long-term treatment plan, especially when medication benefits are preventive rather than immediately felt.
Medication Type Was Not the Main Explanation
The analysis did not find clear adherence differences by medication class. Lithium, valproate, carbamazepine, antidepressants, antipsychotics, first-generation antipsychotics, second-generation antipsychotics, and polytherapy were not significantly different between poor-adherence and good-adherence groups.
The medication-class result needs a narrow reading. It cannot show that all medications are equally easy to take, and it does not erase side effects.
Across the eligible studies, broad medication-class labels did not explain who ended up in the poor-adherence group.
The more actionable takeaway is that adherence support should not wait until a particular medication class is chosen. The higher-risk profile appears earlier:
- Substance use: Screen for cannabis, alcohol, and broader substance-use disorder when treatment is started or changed.
- Insight and functioning: Treat limited illness awareness and impaired daily functioning as adherence risks, not separate issues.
- Clinical course: Watch more closely after psychotic, manic, mixed, or suicidal episodes.
- Social support: Ask whether the person has relationship, family, or practical support for medication routines.
The Evidence Supports Risk Profiling, Not Certainty
The main limitation is evidence quality. No body of evidence was graded high quality. Cannabis use disorder reached moderate quality, but most other correlates were low or very low quality.
Several reasons explain that caution. Many analyses used only a few studies, and some estimates were heterogeneous, meaning study results varied substantially.
Most included studies were observational, so they cannot establish causality. There is also no perfect gold-standard adherence measure for bipolar disorder.
Even with those limits, the pattern is clinically useful. Poor adherence in bipolar disorder was not randomly scattered across the population.
It clustered with substance use, lower insight, poorer functioning, psychotic features, suicide-attempt history, and heavier manic or mixed illness burden.
That argues for early risk profiling. Medication adherence should be discussed as part of bipolar disorder severity, comorbidity, and support needs, not as a separate behavioral checkbox after relapse has already happened.
Citation: DOI: 10.1111/bdi.70127. Bartoli et al. Clinical and sociodemographic correlates of poor medication adherence in people with bipolar disorder: A systematic review and meta-analysis. Bipolar Disorders. 2026;28:e70127.
Study Design: Systematic review and random-effects meta-analysis of observational bipolar disorder studies.
Sample Size: 19 included studies; individual study samples ranged from 44 to 2,205 people.
Key Statistic: Cannabis use disorder was associated with poor medication adherence (OR 2.34, 95% CI 1.79 to 3.07) and was the only correlate graded as moderate-quality evidence.
Caveat: Most evidence was low or very low quality, and the observational design cannot show whether each correlate caused poor adherence or resulted from the same underlying illness burden.