TL;DR: A 2026 systematic review and meta-analysis in Brain, Behavior, & Immunity – Health found that adding celecoxib to antidepressants was linked to lower depressive symptom scores in 7 small trials, but the efficacy evidence was rated very low certainty.
Key Findings
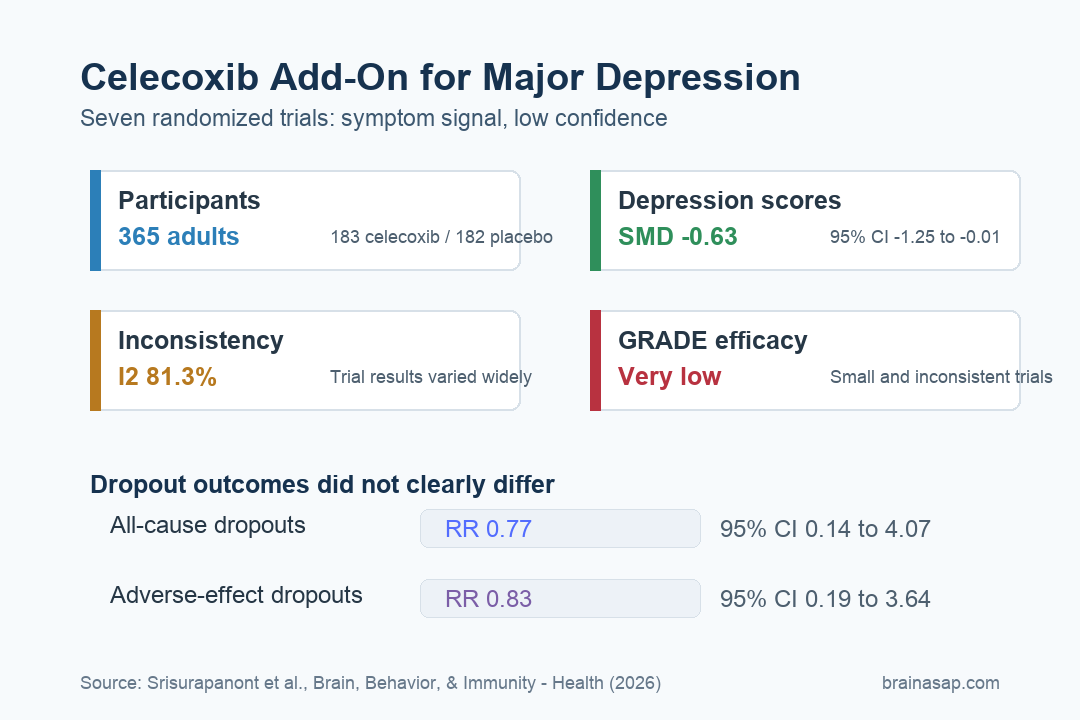
- 7 randomized trials: The meta-analysis included 365 adults with major depressive disorder, with 183 assigned to celecoxib plus antidepressants and 182 assigned to placebo plus antidepressants.
- 400 mg/day common dose: Most trials used celecoxib 400 mg/day for about 6 weeks, usually in patients who were not clearly treatment-resistant.
- Symptom reduction estimate: Adjunctive celecoxib was associated with greater depressive symptom reduction than placebo (SMD = -0.63; 95% CI: -1.25 to -0.01).
- High heterogeneity: The main efficacy analysis had substantial inconsistency (I2 = 81.3%), meaning trial results varied enough to limit confidence in the pooled estimate.
- Dropouts similar: All-cause dropouts (RR = 0.77) and adverse-effect dropouts (RR = 0.83) did not clearly differ between celecoxib and placebo groups.
Source: Brain, Behavior, & Immunity – Health (2026) | Srisurapanont et al.
Inflammation has become a persistent biological lead in depression research. Elevated inflammatory markers do not explain every case of major depressive disorder, but they have been linked with illness chronicity, poor treatment response, and residual symptoms in some patients.
This review focused on celecoxib, a cyclooxygenase-2 (COX-2) inhibitor better known as an anti-inflammatory pain drug. Researchers asked whether adding it to antidepressants improves major depressive disorder outcomes compared with adding a placebo.
Seven Celecoxib Trials Tested Add-On Treatment for Major Depression
The analysis included randomized, double-blind, placebo-controlled trials in adults diagnosed with major depressive disorder. Each trial compared celecoxib plus an antidepressant with placebo plus an antidepressant.
The main outcome was change in depressive symptom severity. Secondary outcomes were all-cause dropouts and dropouts due to adverse effects, which the review used as practical measures of acceptability and tolerability.
The trial set was small and fairly narrow:
- 365 total participants: 183 received celecoxib and 182 received placebo.
- 7 trials: All were published between 2006 and 2024.
- Mostly short treatment: Most trials lasted 6 weeks, with 2 lasting 8 weeks.
- Common dose: Celecoxib was usually given at 400 mg/day.
Background antidepressants varied across studies, including sertraline, escitalopram, fluoxetine, reboxetine, and vortioxetine. 5 trials used the Hamilton Rating Scale for Depression, while 2 used the Montgomery-Asberg Depression Rating Scale.
Depressive Symptoms Were Lower, But the Confidence Interval Was Wide
The pooled efficacy result favored celecoxib. Compared with placebo, adjunctive celecoxib was associated with a depressive symptom reduction of SMD = -0.63, with a 95% confidence interval from -1.25 to -0.01.
That estimate suggests a potentially meaningful antidepressant effect, but it sits close to the edge of statistical uncertainty. The upper bound of the confidence interval is near zero, so the result does not support a strong claim that celecoxib reliably improves depression symptoms across patients.
Several evidence features limit the treatment claim:
- High inconsistency: Trial results varied substantially, with I2 = 81.3% in the main symptom analysis.
- Risk-of-bias concerns: 3 of the 7 trials were judged at high risk of bias for the depressive-symptom outcome.
- Small evidence base: The total sample was far below the size needed for a stable treatment estimate.
- Limited resistant-depression data: Only 1 trial was classified as mainly treatment-resistant depression.
In plain terms, the result points in the expected direction for an anti-inflammatory add-on. It is not strong enough to make celecoxib a routine antidepressant augmentation strategy.
Dropout Results Did Not Show a Clear Tolerability Problem
Safety and tolerability are especially important for add-on depression treatments. A medication that gives a modest symptom benefit but increases discontinuation can be hard to justify in routine care.
In this review, dropout outcomes did not clearly separate celecoxib from placebo. All-cause dropouts had a pooled RR = 0.77, and adverse-effect dropouts had a pooled RR = 0.83.
Those ratios do not show a dropout penalty for celecoxib, but the intervals were wide. The all-cause dropout confidence interval ranged from 0.14 to 4.07, and the adverse-effect dropout interval ranged from 0.19 to 3.64.
The dropout data support 3 narrow points:
- Acceptability: People were not clearly more likely to stop treatment for any reason when celecoxib was added.
- Tolerability: Dropouts due to adverse effects were not clearly higher with celecoxib in short trials.
- Duration limit: These findings mostly reflect 6- to 8-week exposure, not long-term anti-inflammatory use.
Celecoxib also has known medical risks outside psychiatric trials, including cardiovascular, kidney, gastrointestinal, and drug-interaction concerns in some patients. A short depression meta-analysis cannot replace individualized medical risk assessment.
GRADE Ratings Kept the Antidepressant Claim Highly Uncertain
The review used GRADE, a system for rating certainty of evidence. The efficacy outcome ended at very low certainty, even though the data came from randomized trials.
The downgrades were not minor. Efficacy lost confidence because of high risk of bias, serious imprecision, and very serious inconsistency. Acceptability was rated low certainty, while tolerability was rated moderate certainty.
The certainty ratings separate tolerability from efficacy. Celecoxib looked reasonably tolerated over short periods in these trials, while the antidepressant-benefit estimate remained much less secure.
Inflammation-Targeted Depression Treatment Still Needs Better Targeting
The celecoxib finding fits a larger question in psychiatry: whether some patients with depression benefit from targeting immune or inflammatory pathways. The challenge is that major depressive disorder is biologically mixed.
Future trials would be more informative if they tested predefined inflammatory subgroups, measured baseline markers such as C-reactive protein or interleukin-6, and used enough participants to separate treatment responders from noise.
The most useful next studies would answer 3 practical questions:
- Patient selection: Does celecoxib work better in patients with elevated inflammatory markers?
- Clinical durability: Does the symptom difference last beyond the short 6-week window used in most trials?
- Medical tradeoff: Which patients have enough potential antidepressant benefit to justify celecoxib’s nonpsychiatric risks?
For now, the review supports more targeted research on inflammation-guided augmentation. It does not move celecoxib into ordinary depression treatment without stronger evidence from larger, biomarker-informed trials.
Citation: DOI: 10.1016/j.bbih.2026.101277. Srisurapanont et al. Celecoxib adjunct to antidepressants for major depressive disorder: Systematic review and meta-analysis. Brain, Behavior, & Immunity – Health. 2026;55:101277.
Study Design: Systematic review and random-effects meta-analysis of randomized, placebo-controlled adjunctive-treatment trials.
Sample Size: 7 trials with 365 adults with major depressive disorder.
Key Statistic: Depressive symptoms favored celecoxib plus antidepressants over placebo plus antidepressants (SMD = -0.63; 95% CI: -1.25 to -0.01; I2 = 81.3%).
Caveat: Efficacy evidence was rated very low certainty because the trials were small, inconsistent, and included several high-risk-of-bias studies.