TL;DR: A 2026 study in Neuropsychopharmacology found that decision-making measures from a stop-signal task, especially evidence accumulation, predicted cigarette and cannabis use better than stop-signal reaction time (SSRT), a common estimate of response inhibition.
Key Findings
- More than 1,000 young adults: The analysis used IMAGEN cohort stop-signal task data from 1,256 participants at age 19 and 1,089 participants at age 23.
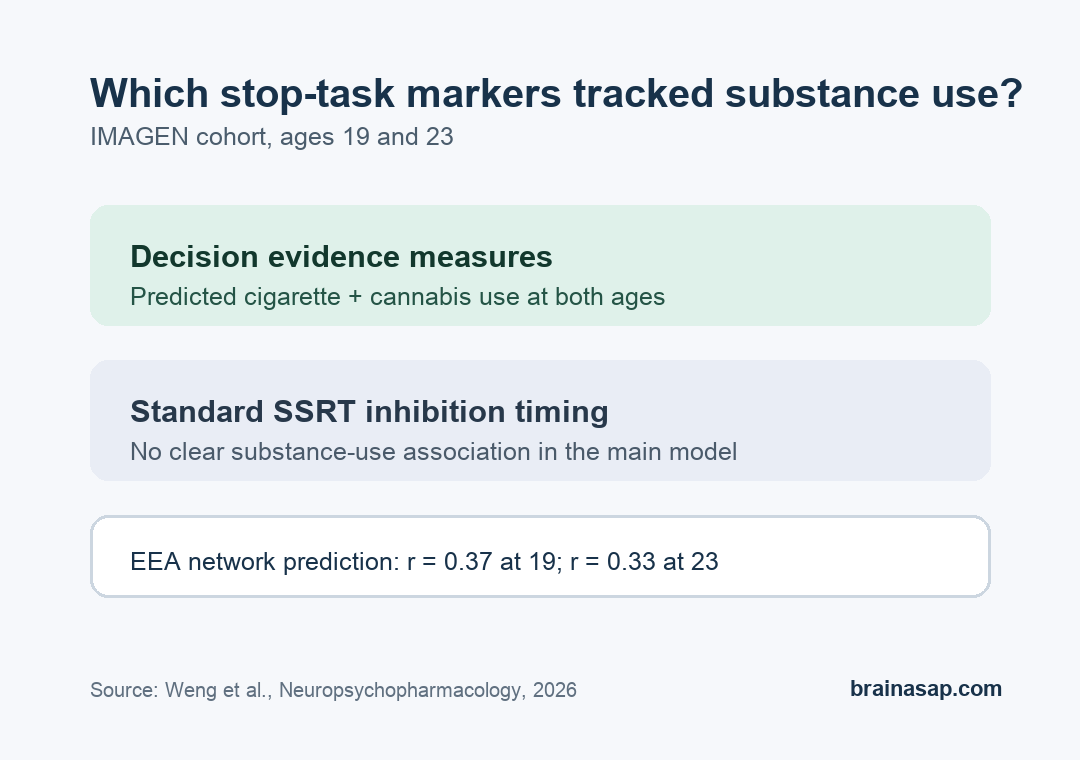
- Decision-making beat inhibition: Model parameters tied to evidence accumulation, decision threshold, and go failures predicted cigarette and cannabis use, while inhibition measures did not show comparable links.
- Standard SSRT was weaker: SSRT, a conventional stop-task inhibition score, had no apparent substance-use association in the main model.
- Brain connectivity supported the pattern: Functional brain networks predicted evidence accumulation at both ages, with correlations of r = 0.37 at 19 and r = 0.33 at 23.
- Not a diagnostic test: The findings point to modest group-level risk markers, not a tool that can identify who will develop a substance use disorder.
Source: 2026 study in Neuropsychopharmacology.
Stop-Signal Modeling Separated Decision Speed From Inhibition
The stop-signal task is often used to study self-control. Participants respond quickly to a go cue, then try to withhold that response when a stop cue appears.
A common summary score is stop-signal reaction time, or SSRT, which estimates how long the stopping process takes.
Weng and researchers working with the IMAGEN cohort asked whether that familiar inhibition score was too narrow. They used a computational model called Racing Diffusion Ex-Gaussian ABCD, or RDEX-ABCD, to split task performance into several latent decision processes rather than treating the task as one inhibition number.
The model separated three especially relevant pieces of behavior:
- Evidence accumulation: how efficiently a participant gathered task-relevant information before choosing a response.
- Decision threshold: how cautious the participant was before committing to a response.
- Go failure probability: how often attention or response execution failed on ordinary go trials.
This distinction changes the interpretation because substance use vulnerability is often described as poor inhibition. The study tested a sharper possibility: some of the useful information may come from general decision-making quality, not only from the ability to stop an already-started action.
Evidence Accumulation Predicted Cigarette and Cannabis Use
The analysis used stop-signal data from 1,256 participants at age 19 and 1,089 participants at age 23. Participants also completed Timeline Followback assessments.
Those assessments measured recent alcohol, cigarette, cannabis, and other drug use. The main substance-use outcome discussed in the results combined cigarette and cannabis use.
Researchers used elastic net regression, a machine-learning method that can handle related predictors, to test whether the 11 model parameters predicted substance-use scores. For cigarette plus cannabis use, the models performed better than random-label permutation tests at both ages, with P values below 0.001.
The clearest predictors were not the standard inhibition markers. At age 19, the largest feature weights came from go failure probability, evidence accumulation, and decision threshold.
At age 23, the same three parameters again ranked highest. Each was selected in 100 of 100 repeated elastic net runs at both ages.
The pattern was narrower than a broad substance-use claim:
- Cigarette and cannabis use: decision parameters showed significant prediction at both ages.
- Alcohol use: model parameters did not show significant associations in the reported tests.
- Other drug use: the same null pattern appeared for the other-drug factor.
This result should not be read as showing that one task score causes cigarette or cannabis use. The model found reproducible, modest links between decision evidence quality and recent cigarette/cannabis behavior in a large young-adult cohort.
Brain Networks Tracked Decision Parameters More Than Standard Inhibition
The study also linked task parameters to functional brain connectivity. Researchers used connectome-based predictive modeling to ask whether whole-brain networks could predict the model-derived parameters from task-related functional MRI (fMRI) data.
Combined networks significantly predicted evidence accumulation, decision threshold, and go failure probability at both ages. Evidence accumulation had the strongest network prediction among these measures, with r = 0.37 at age 19 and r = 0.33 at age 23.
Network strength also added some substance-use context. At age 23, evidence-accumulation network strength correlated with cigarette plus cannabis use (rho = -0.12, P = 2.57E-04).
Decision-threshold network strength also correlated with that factor (rho = -0.11, P = 4.99E-04). By contrast, network strength for standard and RDEX-derived SSRT did not show significant cigarette/cannabis correlations.
In practical terms, the brain results point in the same direction as the behavior model:
- Decision evidence measures: showed more consistent behavioral and neural links with cigarette/cannabis use.
- Response-inhibition timing: was measurable, but less informative for substance-use associations in this sample.
- Network reliability: evidence-accumulation network strength was correlated across ages 19 and 23 (R = 0.60), suggesting relatively stable individual differences.
Risk Markers Remain Far From a Clinical Test
The study is useful because it challenges a common shortcut. Poor inhibition is a familiar explanation for substance use risk, but this analysis suggests noisy or inefficient decision-making may be the more reliable task-derived marker in late adolescence and early adulthood.
That interpretation still needs restraint. The effect sizes were modest, and the substance-use measures were recent-use factors rather than clinical diagnoses.
The design also cannot prove that low evidence accumulation caused later substance use. The results are best read as a computational-neuroscience clue about vulnerability, not as a screening tool.
The clinical value, if it develops, would likely come from combining measures. A future risk model might use decision-task parameters, symptoms, family history, environment, and longitudinal substance-use trajectories.
A single stop-signal model parameter is not enough.
For now, the sharper takeaway is that general decision-making mechanisms may deserve at least as much attention as inhibition speed when researchers study why some young adults are more vulnerable to cigarette and cannabis use.
Citation: DOI: 10.1038/s41386-026-02401-6. Weng et al. Model-based analysis of stop-signal data reveals robust neural and clinical correlates of evidence accumulation but not inhibition. Neuropsychopharmacology. 2026.
Study Design: Longitudinal cohort analysis using computational modeling of stop-signal task behavior and task fMRI connectivity.
Sample Size: 1,256 IMAGEN participants at age 19 and 1,089 participants at age 23 for model estimation.
Key Statistic: Evidence-accumulation brain-network prediction reached r = 0.37 at age 19 and r = 0.33 at age 23; SSRT network strength did not significantly correlate with cigarette/cannabis use.
Caveat: The associations were modest and based on recent-use factors, not clinical substance use disorder diagnoses.