TL;DR: A 2026 retrospective chart review in Acta Psychiatrica Scandinavica found that a psychiatrist-led metabolic clinic helped 132 of 378 patients with severe mental illness lose at least 5% of baseline body weight over 12 months.
Key Findings
- Clinic outcomes were tracked: Researchers analyzed 378 people treated at the Centre for Addiction and Mental Health metabolic clinic from 2016 to 2023.
- 37.5% lost at least 5% of body weight: The primary outcome was clinically meaningful weight loss over a 12-month clinic window.
- Metformin had the largest treatment group: 79 of 214 patients receiving add-on metformin reached the 5% weight-loss threshold.
- Semaglutide looked strongest but small: 7 of 11 patients receiving add-on semaglutide lost at least 5% of baseline weight.
- The design was observational: Chart data, missing values, uneven treatment groups, and clinical heterogeneity limit causal interpretation.
Source: Acta Psychiatrica Scandinavica (2026) | Stogios et al.
Antipsychotic-associated weight gain is not a cosmetic side effect. For people with severe mental illness, metabolic risk sits inside a larger mortality gap that includes diabetes, cardiovascular disease, medication exposure, poverty, fragmented care, and under-treated physical health.
This Canadian chart review tested a practical question: what happens when metabolic care is built into a psychiatric setting instead of being left for a separate referral system?
A Psychiatrist-Led Clinic Treated Metabolic Risk Inside Mental Health Care
Researchers reviewed all patients who attended the Mental Health and Metabolism Clinic at the Centre for Addiction and Mental Health in Toronto between 2016 and 2023. The clinic used an integrated model that combined measurement-based monitoring, lifestyle counseling, and medication options for psychotropic-associated metabolic dysfunction.
The study population was clinically broad. Diagnoses included schizophrenia, schizoaffective disorder, psychosis-spectrum conditions, bipolar disorder, major depressive disorder, and multiple diagnoses.
Many patients were taking antipsychotics, including agents commonly associated with weight and metabolic effects.
- Primary measure: The percentage of patients who lost at least 5% of baseline body weight over 12 months.
- Additional threshold: Researchers also tracked at least 7% weight loss, a stricter benchmark.
- Secondary measures: Body mass index, waist circumference, glucose markers, lipids, insulin resistance, and other metabolic parameters were reviewed when chart data were available.
The main result was direct. Across the full sample, 132 of 378 patients, or 37.5%, lost at least 5% of their baseline body weight during the 12-month study period.
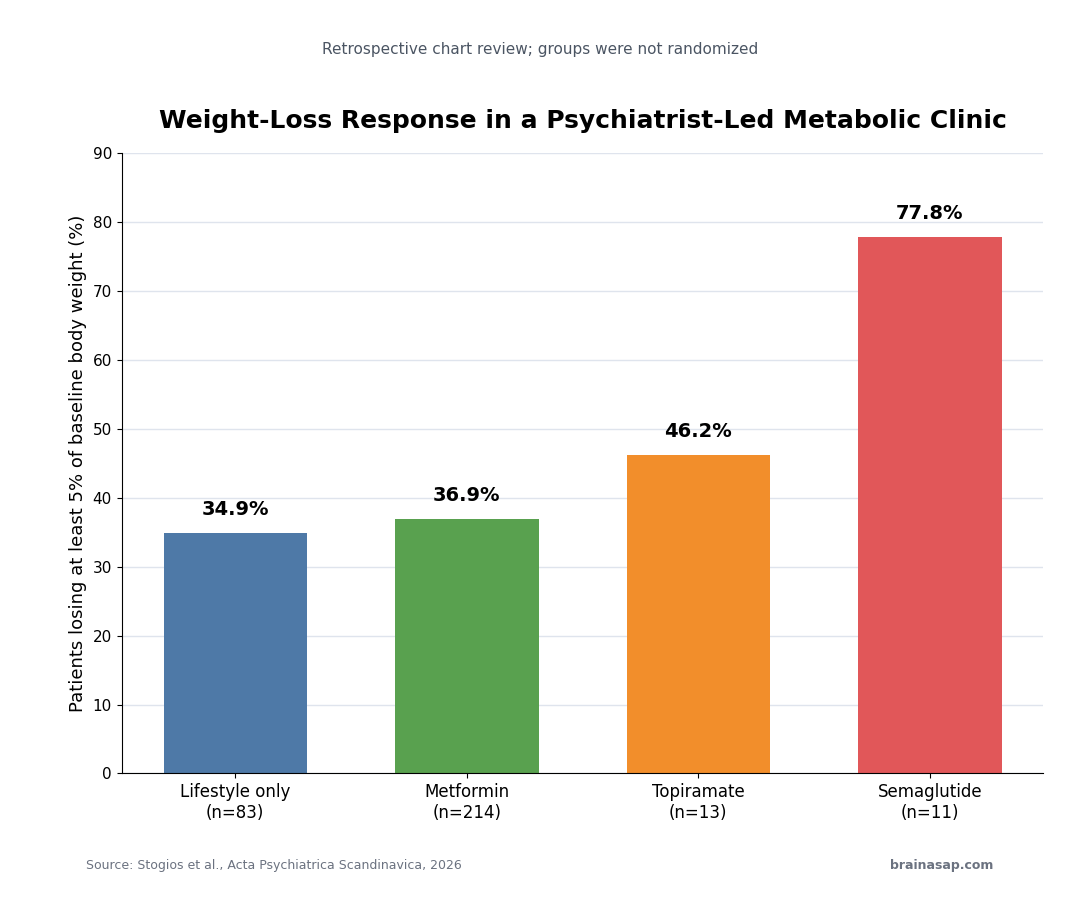
Weight Loss Varied Across Lifestyle, Metformin, Topiramate, and Semaglutide
The clinic did not use one uniform intervention. Patients received lifestyle-only support or add-on medications such as metformin, topiramate, and semaglutide, depending on clinical need and treatment decisions.
The 5% weight-loss threshold appeared in every major intervention group, but the denominators were very different:
- Lifestyle-only care: 29 of 83 patients, or 34.9%, lost at least 5% of baseline body weight.
- Add-on metformin: 79 of 214 patients, or 36.9%, reached the same threshold.
- Add-on topiramate: 6 of 13 patients, or 46.2%, reached at least 5% weight loss.
- Add-on semaglutide: 7 of 11 patients, or 77.8%, reached at least 5% weight loss.
The semaglutide signal is the easiest number to notice, but it should not be read as a clean head-to-head comparison.
Only 11 patients were in that add-on group, and the study was not randomized.
The safer interpretation is that GLP-1-based treatment looked promising inside this clinic. Larger controlled studies are still needed to estimate its true effect in this population.
The Mean Weight Change Was Modest, but the Threshold Result Still Helps
Across all interventions, researchers found a significant effect of clinic care on body weight over time. The mean change at 12 months was -1.24 kg, with a standard deviation of 1.45 kg.
That mean can sound modest because it averages very different clinical trajectories. Some patients lost a clinically meaningful amount, while others lost less, stayed stable, or likely gained.
The 5% threshold is useful because it identifies the subgroup whose weight change is large enough to plausibly affect cardiometabolic risk.
The paper also reported a heuristic number needed to treat. Under a conservative assumption that untreated patients would not lose weight, the estimated number needed for one patient to achieve at least 5% weight loss was:
- 3 patients for lifestyle-only care, metformin, and topiramate.
- 2 patients for semaglutide.
The researchers were careful about that calculation. Because this was not a randomized trial, those values are not equivalent to trial-derived NNTs.
They are best read as a clinical shorthand for the observed clinic outcomes, not as proof of comparative efficacy.
Psychiatric Settings May Be the Right Place to Treat Metabolic Side Effects
The strongest practical message is not that one medication won. It is that metabolic care can be organized inside mental health services, where antipsychotic prescribing, symptom stability, adherence concerns, and cardiometabolic monitoring can be discussed together.
This structure helps because people with severe mental illness often face barriers to routine medical care.
A separate referral for weight, glucose, lipids, or cardiovascular risk can easily disappear behind transportation, appointment burden, symptoms, medication changes, or stigma.
A psychiatric metabolic clinic changes the workflow. Weight and labs are monitored as part of psychiatric care, while medication choices can account for both mental-health stability and metabolic burden.
- Monitoring becomes systematic: Body weight, waist circumference, glucose, and lipid markers can be checked instead of assumed.
- Medication decisions become coordinated: Clinicians can address weight-gain risk without destabilizing psychiatric treatment.
- Escalation becomes easier: Lifestyle support, metformin, topiramate, or GLP-1 treatment can be considered in a stepwise way.
That integrated structure is the part of the study with the clearest health-system relevance.
Retrospective Chart Data Cannot Prove the Clinic Caused the Weight Loss
The study has important limits. Chart reviews depend on what clinicians recorded, so missing values are expected.
Treatment groups were uneven, with add-on metformin representing more than half of the sample and semaglutide representing only a small group.
The patients also differed by diagnosis, medication exposure, illness chronicity, and other clinical variables. Those differences make it hard to separate the effect of the clinic from selection factors, medication changes, motivation, follow-up intensity, or baseline metabolic risk.
Attrition is also important. The paper reported that 135 of 378 patients, or 35.7%, withdrew from the clinic with no future visits.
That is not unusual in real-world psychiatric services, but it affects how confidently the results can be generalized.
The best reading is therefore specific. In one large real-world psychiatric metabolic clinic, a meaningful minority of patients with severe mental illness achieved clinically relevant weight loss over 12 months.
The finding supports integrated metabolic care, but it does not replace randomized comparisons of specific interventions.
Citation: DOI: 10.1111/acps.70093. Stogios et al. Effectiveness of a Psychiatrist-Led Clinic for Metabolic Health in Severe Mental Illness: A Retrospective Chart Review Study. Acta Psychiatrica Scandinavica. 2026;154:74-88.
Study Design: Retrospective chart review of a psychiatrist-led metabolic clinic at the Centre for Addiction and Mental Health.
Sample Size: 378 patients with severe mental illness treated between 2016 and 2023.
Key Statistic: 132 of 378 patients, or 37.5%, lost at least 5% of baseline body weight over 12 months.
Caveat: Observational chart data, missing values, uneven treatment groups, and clinic attrition limit causal claims.