TL;DR: A 2026 preprint on medRxiv found that adding 24 IU intranasal oxytocin before 4 mindfulness-based group therapy sessions was linked to larger clinician-rated negative-symptom improvements in a small schizophrenia spectrum disorder pilot trial.
Key Findings
- Oxytocin arm showed the main signal: The OXYMIND pilot assigned 26 outpatients to oxytocin plus mindfulness-based group therapy and 21 to placebo plus the same therapy.
- 4 MBGT sessions used: Each group received 4 weekly mindfulness-based group therapy sessions, with oxytocin or placebo nasal spray given 30 minutes before each session.
- PANSS-N improved in oxytocin group: Positive and Negative Syndrome Scale negative-subscale scores fell from baseline to follow-up with d = -0.77 in the oxytocin group.
- BNSS also favored oxytocin: Brief Negative Symptom Scale total scores showed a follow-up between-group difference of -5.11 points favoring oxytocin plus therapy.
- Pilot limits remain: The preprint was small, monocentric, outpatient-only, not peer reviewed, and not corrected for multiple testing.
Source: medRxiv (2026) | Zierhut et al.
Negative symptoms in schizophrenia spectrum disorders include reduced motivation, blunted emotional expression, social withdrawal, and limited speech output. These symptoms often persist even when hallucinations or delusions are controlled, and they are difficult to treat with standard medication alone.
The OXYMIND trial tested a specific augmentation idea: pair intranasal oxytocin, a hormone involved in social salience and affiliation, with a supportive group therapy context designed for people with psychosis.
4 Sessions Paired 24 IU Oxytocin With Mindfulness Group Therapy
Researchers at Charite in Berlin ran a triple-blind randomized pilot trial in outpatients with schizophrenia spectrum disorders. Participants, psychotherapists, and clinical raters were blinded to whether the nasal spray contained oxytocin or placebo.
The treatment window was short. Participants attended 4 weekly 60-minute mindfulness-based group therapy (MBGT) sessions, each preceded by 6 bursts of nasal spray about 30 minutes before the session.
- Oxytocin arm: 26 participants received 24 IU synthetic oxytocin before MBGT.
- Placebo arm: 21 participants received saline spray before the same MBGT program.
- Assessment schedule: Symptoms were measured at baseline, after the intervention, and again at a 4-week follow-up.
The main clinical target was negative symptoms, not general distress. The primary measure was the Positive and Negative Syndrome Scale negative subscale (PANSS-N), a clinician-rated schizophrenia symptom scale focused on negative-symptom items.
PANSS-N and BNSS Scores Improved Mainly in the Oxytocin Group
On the PANSS-N, scores decreased significantly only in the oxytocin plus MBGT group. From baseline to post-intervention, the change was -2.27 points with d = -0.74; from baseline to follow-up, the change was -2.75 points with d = -0.77.
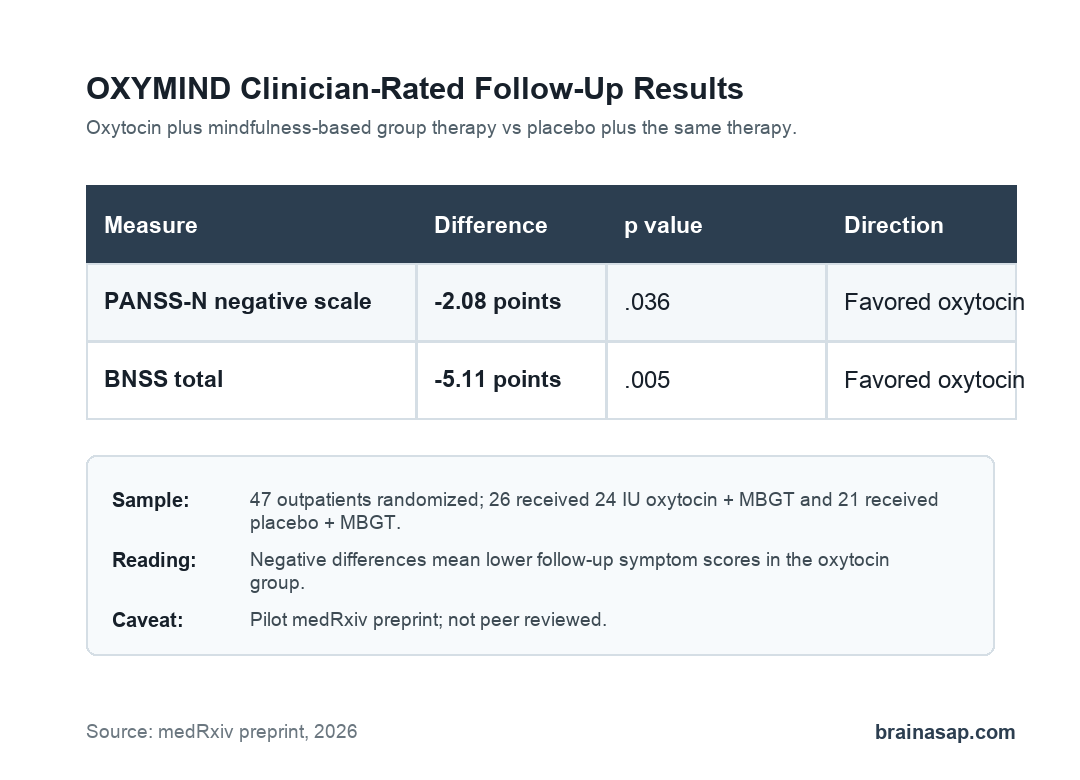
The placebo plus MBGT group showed smaller, non-significant PANSS-N changes. At the 4-week follow-up, the between-group model favored oxytocin by -2.08 points, with p = .036 and a small effect size.
The second-generation clinician scale told a similar story. The Brief Negative Symptom Scale (BNSS), which measures domains such as anhedonia, asociality, avolition, blunted affect, and alogia, improved significantly only in the oxytocin group.
- BNSS post-intervention: Oxytocin plus MBGT changed by -4.53 points from baseline, with d = -0.88.
- BNSS follow-up: Oxytocin plus MBGT changed by -5.05 points from baseline, with d = -0.91.
- BNSS between-group contrast: At follow-up, the difference was -5.11 points favoring oxytocin plus MBGT.
Clinician-Rated Benefits Did Not Fully Match Self-Rated Symptoms
The self-rated measure was the Self-Evaluation of Negative Symptoms Scale (SNS). Unlike PANSS-N and BNSS, total SNS scores did not show significant within-group or between-group improvement.
That split is important because negative symptoms can be hard for patients to rate consistently. Insight, cognition, emotional awareness, and the difference between internal experience and observable behavior can all affect self-report.
Other outcomes also moved in the oxytocin group. PANSS total, positive, and general symptom scores improved within that group, and PANSS total scores favored oxytocin at follow-up.
Depressive symptoms did not significantly improve, which reduces the chance that the negative-symptom pattern was only a depression effect.
Successful Blinding and High Attendance Support Feasibility
The trial was small, but it did show that the combined intervention was feasible in an outpatient psychosis sample. Retained participants completed 95.63% of MBGT sessions, and the overall dropout rate was 14.89%.
Safety findings were also reassuring for a pilot. No serious adverse events occurred, and only 1 dropout in the oxytocin group was considered potentially treatment-related because of transient nasal irritation.
- Blinding check: Among participants reached after completion, allocation guesses indicated successful blinding.
- Therapy acceptability: Attendance stayed high across 13 4-session MBGT cycles.
- Clinical setting: Most participants were recruited from an outpatient psychiatric clinic, making the test relevant to routine care but still limited to one center.
Small Pilot Design Limits OXYMIND Treatment Claims
The strongest practical reading is cautious: oxytocin plus MBGT produced promising clinician-rated negative-symptom findings, but the trial does not yet support a treatment recommendation.
Several limits matter before interpreting the effect as clinically established:
- Small sample: Only 47 participants were randomized, so estimates can shift in a larger trial.
- Single site: The study was monocentric and outpatient-only, which limits generalizability.
- No multiple-testing correction: Several outcomes and subscales were tested, increasing the need for replication.
- One dose: The trial tested 24 IU oxytocin, so it cannot identify the best dose or dosing schedule.
- Preprint status: The source was posted on medRxiv and had not been certified by peer review.
If larger multicenter trials reproduce the PANSS-N and BNSS findings, oxytocin-augmented mindfulness therapy could become a more serious candidate for hard-to-treat negative symptoms in schizophrenia spectrum disorders. For now, OXYMIND is best read as a carefully blinded pilot signal that justifies a larger test.
Citation: DOI: 10.64898/2026.07.01.26356996. Zierhut et al. The Combination of Oxytocin with Mindfulness-Based Group Therapy Reduces Negative Symptoms in Schizophrenia Spectrum Disorders: A Triple-Blind, Placebo-Controlled, Randomized, Controlled Clinical Pilot Trial (OXYMIND). medRxiv. 2026.
Study Design: Triple-blind, placebo-controlled, randomized clinical pilot trial.
Sample Size: 47 outpatients with schizophrenia spectrum disorders.
Key Statistic: At 4-week follow-up, PANSS-N differed by -2.08 points and BNSS total differed by -5.11 points, both favoring oxytocin plus MBGT.
Caveat: Small single-center preprint without peer review or multiple-testing correction.