TL;DR: Chronic insomnia fragments REM sleep through persistent hyperarousal, preventing emotional memory consolidation and creating a vicious cycle that breeds depression—but cognitive-behavioral therapy for insomnia can break the cycle faster than antidepressants alone.
Insomnia has a hidden mechanism. You lie awake for hours, but the real problem isn’t the wakefulness—it’s what happens to REM sleep, the stage responsible for emotional healing.
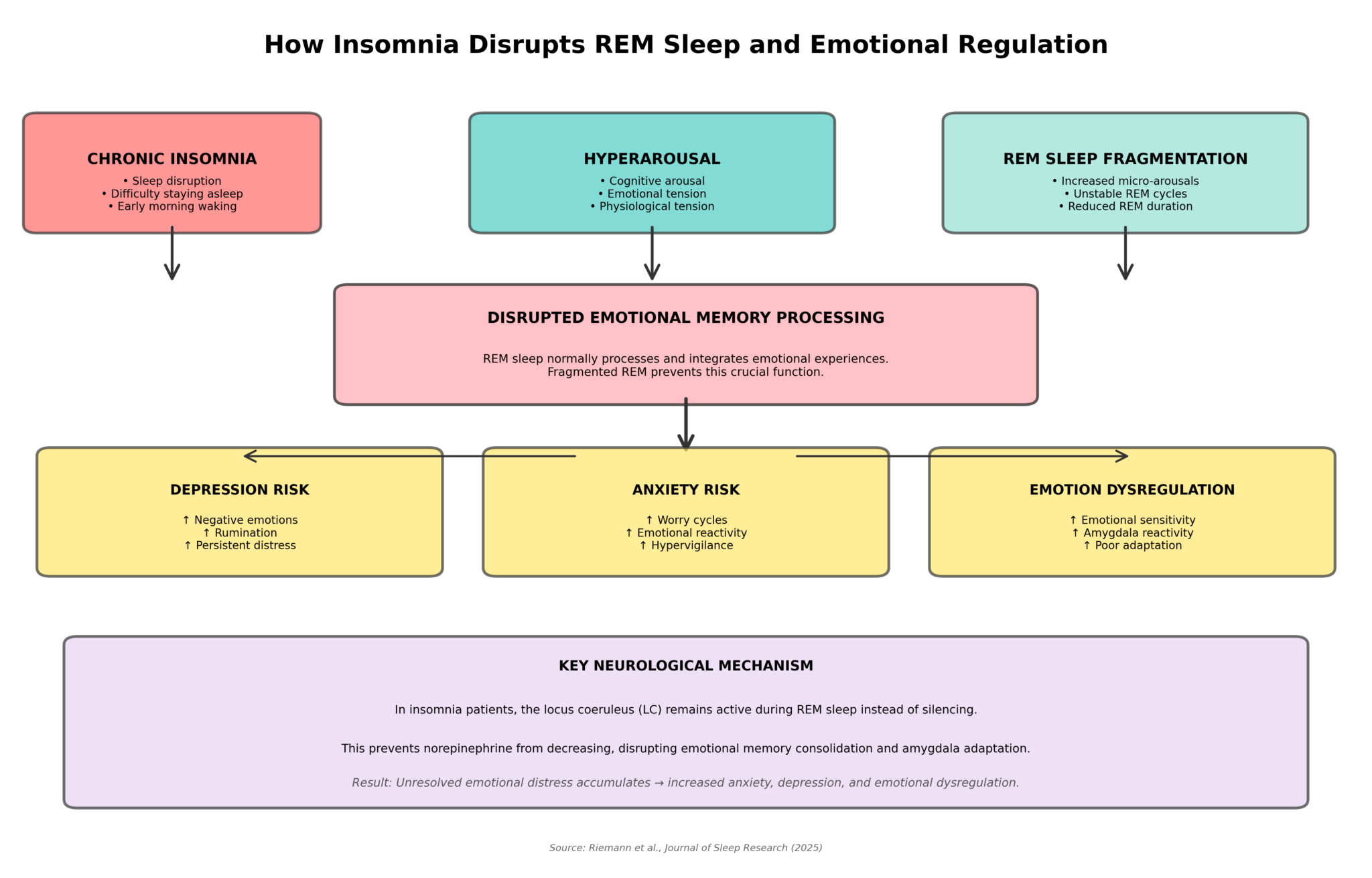
A landmark review from Dieter Riemann and colleagues at the University of Freiburg synthesizes two decades of neuroscience explaining how chronic insomnia fragments REM sleep, preventing emotional memory processing and breeding depression. This mechanism is now clear and measurable.
This reframing shifts everything. Insomnia isn’t just a symptom of depression—it’s a mechanism that generates it.
Key Findings
- REM sleep becomes fragmented: Insomnia patients show dramatically elevated micro-arousals (brief partial awakenings) specifically during REM sleep, the 20–25% of the night devoted to emotional memory processing and emotional regulation. Non-REM sleep remains largely intact; REM becomes the vulnerable target.
- The brain’s arousal system won’t shut off: The locus coeruleus—a cluster of 16,000 neurons that produces norepinephrine, the brain’s primary alertness chemical—fails to fully silence during REM sleep in insomnia patients. This persistent norepinephrine blocks the neurochemical conditions necessary for emotional memory consolidation.
- Emotional memories never get processed: Without quiet, sustained REM sleep, the amygdala (the brain’s emotional center) cannot downregulate or integrate distressing memories. Psychological stress that should fade overnight instead accumulates, night after night.
- Hyperarousal operates on three fronts simultaneously: Cognitive (racing thoughts, rumination about sleep), emotional (heightened threat sensitivity), and physiological (elevated cortisol, sympathetic activation) hyperarousal converge to destabilize REM and prevent emotional regulation.
- You feel awake while actually sleeping: When awakened from fragmented REM, insomnia patients report feeling awake significantly more than good sleepers awakened from the same REM stage. Fragmented REM produces phenomenological wakefulness—the conscious experience of being awake even during sleep.
- A vicious bidirectional cycle: Longitudinal studies found that nights with worse sleep disruption predicted higher emotional reactivity the next day, while days with negative emotions predicted worse sleep that night. Fragmented REM → emotional dysregulation → worse sleep → more fragmented REM.
Source: Journal of Sleep Research (2025) | Riemann et al.
The Bigger Picture: A New Model of Insomnia and Mental Health
For decades, insomnia and depression were treated as separate disorders. This review reshapes that model. Chronic insomnia fundamentally disrupts REM sleep architecture. This fragmentation prevents emotional memory consolidation, allowing distress to accumulate rather than resolve.
Over time, the brain’s emotional center becomes increasingly sensitized. Depression and anxiety follow inevitably.
This reframing has profound implications. Targeting REM sleep stability might treat both insomnia and mood disorders simultaneously. Early evidence supports this: CBT-I (cognitive-behavioral therapy for insomnia) produces mood improvements within weeks—faster than antidepressants alone, without side effects.
The amygdala, given sustained quiet REM sleep, can downregulate overnight. The vicious cycle can break.
A Brain That Never Downregulates
The fundamental problem in chronic insomnia isn’t failing to fall asleep—it’s failing to downregulate arousal. Brain imaging shows insomnia patients remain metabolically hyperactive even during sleep. This persistent hyperarousal operates on three simultaneous tracks:
- Cognitive: Racing thoughts, sleep-focused worry, rumination
- Emotional: Heightened threat sensitivity, poor emotional regulation
- Physiological: Elevated cortisol, sympathetic activation, increased heart rate
The result is a brain locked in vigilance when it should rest. REM sleep is already the brain’s most aroused sleep stage. Layer chronic hyperarousal on top, and REM destabilizes.
Micro-arousals—brief partial awakenings—spike specifically during REM in insomnia patients. Non-REM sleep remains relatively stable. REM becomes the vulnerable stage and the defining physiological feature of chronic insomnia.
When the Alertness System Forgets to Shut Off
Deep in the brainstem lives the locus coeruleus, a cluster of 16,000 neurons controlling wakefulness. These neurons produce norepinephrine, the brain’s primary alert chemical. During healthy REM sleep, this system nearly shuts down.
Norepinephrine levels plummet. This chemical silence allows synaptic plasticity—the rewiring underlying emotional memory consolidation. Without it, psychological stress stays fresh and emotionally charged.
In insomnia patients, the locus coeruleus fails to silence during REM. Norepinephrine remains elevated, preventing the chemical conditions necessary for emotional consolidation.
The emotional system needs sustained, quiet REM sleep to downregulate. Night after night, without that window, it becomes increasingly sensitized and reactive, locked in alarm.
The Neuroscience Behind “I Never Actually Fall Asleep”
Every sleep researcher knows the insomnia paradox. Connect a patient to polysomnography—the gold-standard measurement via EEG, eye movement, and muscle tone—and they report being awake far longer than the recordings show. Patient reports 2 hours awake; the machine records 45 minutes.
For years, this seemed like anxiety distortion. Then researchers performed a critical experiment: they awakened insomnia patients directly from REM sleep and asked if they felt asleep or awake. Insomnia patients reported feeling awake significantly more than good sleepers awakened from identical REM sleep. When both groups were awakened from non-REM sleep, this difference disappeared.
The insight was revolutionary. Fragmented REM creates a phenomenological mismatch—the brain and body are technically sleeping, but conscious experience feels like wakefulness. Micro-arousals spike in REM, fragmenting the dream state into consciousness-like episodes. Each fragment feels like waking.
Cumulatively, fragmented REM feels like being awake all night, even when the machine shows reasonable sleep. This false consciousness feeds anticipatory anxiety (“I won’t sleep tonight”), which further destabilizes REM. Insomnia patients feel that way because their REM sleep is genuinely fragmented into wakefulness-like consciousness.
Why Insomnia Predicts Depression (And It’s Not What You Think)
The relationship between insomnia and depression is among the most robust findings in all sleep research. The evidence is unidirectional on multiple fronts:
- Elevated depression risk: Insomnia patients carry substantially elevated lifetime risk of depression.
- Prospective prediction: Insomnia predicts future major depressive episodes.
- Bidirectional for anxiety: The same pattern holds for anxiety disorders.
For decades, researchers asked the wrong question: is depression causing insomnia, or is insomnia causing depression? The answer is both. The mechanism is REM fragmentation preventing emotional memory consolidation.
Longitudinal studies found a striking bidirectional cycle: nights with worse sleep predicted heightened emotional reactivity the next day. Days with negative emotions predicted worse sleep that night. This creates the vicious loop.
Distress accumulates rather than fades.
Neuroimaging findings: Brain imaging confirms this mechanism at the circuit level:
- Healthy sleepers show overnight habituation: The amygdala downregulates overnight, becoming less reactive.
- Insomnia patients show stuck reactivity: The emotional system remains locked in its reactive state. The locus coeruleus fails to silence, never getting the window to downregulate.
- Progressive sensitization: Without adequate REM sleep, the emotional system becomes increasingly sensitized. Vulnerability to depression and anxiety accelerates.
What This Means for Treatment
- Screen for mood disorders in every insomnia patient. Insomnia without concurrent mood or anxiety symptoms is rare. When patients present with “just insomnia,” ask about subthreshold depression. Mood screening should be routine.
- Treat sleep fragmentation, not just the mood. When depression emerges with chronic insomnia, REM fragmentation is likely driving the mood symptoms. Use cognitive-behavioral therapy for insomnia (CBT-I), the evidence-based first-line approach that addresses hyperarousal.
- Choose sleep medications carefully. Traditional sedatives like benzodiazepines suppress REM sleep, ironically worsening the REM fragmentation driving mood dysregulation. Medications that preserve REM integrity (melatonin, certain newer agents) may be preferable. But behavioral approaches remain first-line.
- Sleep recovery may work faster than mood medication. Because fragmented REM prevents emotional consolidation, fixing the sleep may rapidly improve mood. Early trials of CBT-I show mood benefits within weeks—often faster than antidepressants alone, without side effects.
- Acceptance beats suppression at the pillow. Insomnia patients who suppress pre-sleep worries paradoxically intensify the dysregulation cycle. Pre-sleep acceptance-based strategies—acknowledging worries without fighting them—may break the cycle more effectively.
Full Citation: Riemann D, Dressle RJ, Benz F, et al. Chronic insomnia, REM sleep instability and emotional dysregulation: A pathway to anxiety and depression? Journal of Sleep Research. 2025;34(2):e14252. DOI: 10.1111/jsr.14252
Study Type: Comprehensive narrative review synthesizing neurobiological mechanisms linking insomnia, REM sleep fragmentation, and emotional dysregulation to depression and anxiety disorders
Key Mechanism: REM sleep instability (elevated micro-arousals during REM) prevents emotional memory consolidation by failing to silence the locus coeruleus (LC) and downregulate the amygdala, allowing emotional distress to accumulate across nights
Clinical Implication: Cognitive-behavioral therapy for insomnia (CBT-I) targeting hyperarousal may simultaneously treat insomnia and comorbid mood/anxiety disorders by restoring REM sleep stability
Lead Authors: Dieter Riemann (University of Freiburg), with international collaborators from Oxford, University of Pennsylvania, and the German Center for Mental Health