TL;DR: A 2026 systematic review and meta-analysis in BMC Psychiatry reported that olanzapine produced a numerically higher body mass index gain in anorexia nervosa trials, but the pooled randomized evidence remained small, heterogeneous, and not statistically significant.
Key Findings
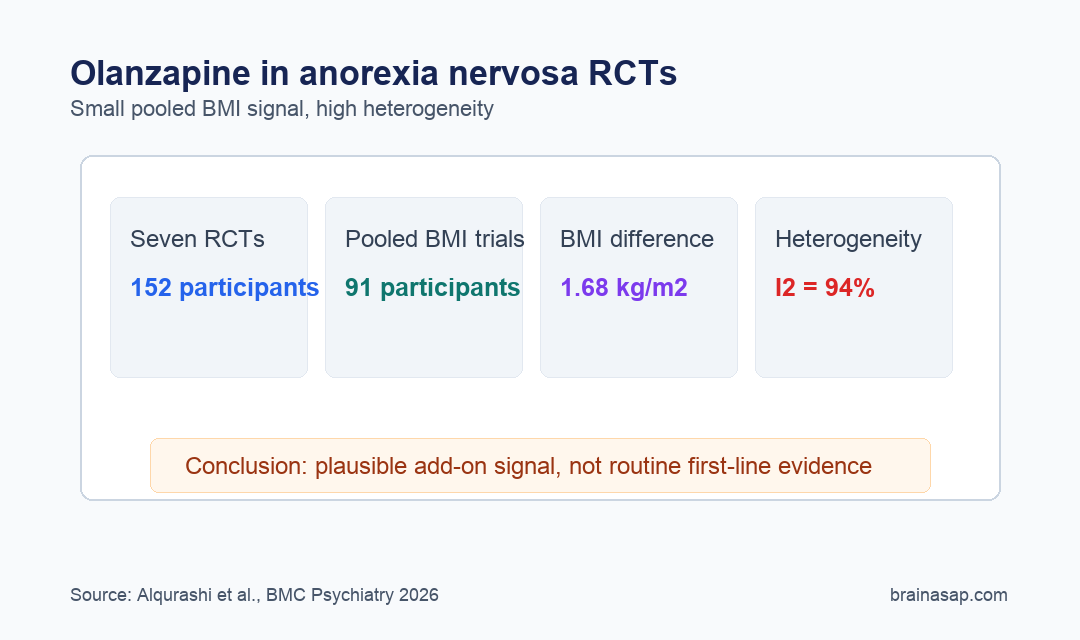
- 7 RCTs included: The review found 7 randomized controlled trials with 152 people treated for anorexia nervosa.
- 4 trials pooled: Only 4 trials, totaling 91 participants, had enough body mass index data for the main meta-analysis.
- 1.68 kg/m2 BMI difference: Olanzapine favored higher BMI gain by a mean difference of 1.68 kg/m2, but the 95% confidence interval ranged from 0.82 to 4.18 and did not produce a statistically significant pooled finding.
- 94% heterogeneity: The main pooled analysis had I2 = 94%, meaning the trial results varied too much for a simple treatment conclusion.
- Moderate certainty: The evidence was rated moderate, with concerns about small samples, mixed trial designs, and risk-of-bias issues in several studies.
Source: BMC Psychiatry (2026) | Alqurashi et al.
Olanzapine, an atypical antipsychotic, is sometimes considered as an add-on treatment in anorexia nervosa because weight restoration is difficult and obsessive eating-disorder thoughts can remain severe during care. The clinical issue is whether randomized anorexia nervosa trials show enough benefit for routine use.
This review narrowed the evidence to randomized controlled trials and treated body mass index (BMI), weight divided by height squared, as the main pooled outcome.
Olanzapine Favored BMI Gain, But the Randomized Evidence Stayed Small
Researchers searched Medline, ClinicalTrials.gov, Scopus, and the Cochrane Database through August 22, 2024. After screening 207 records, they included 7 randomized controlled trials of olanzapine in anorexia nervosa.
The trials were not large. Across all 7, the review counted 152 participants, with individual trial sizes ranging from 15 to 50 people.
Only 4 trials, with 91 participants, reported BMI change with enough detail to enter the meta-analysis.
- Primary outcome: Change in BMI, not a broad improvement score.
- Eligible designs: Randomized controlled trials only; observational studies, case reports, single-arm studies, and protocols were excluded.
- Comparators: Placebo, therapy, or other drug treatment, including aripiprazole and chlorpromazine in some trials.
The pooled BMI result moved in olanzapine’s direction. The mean difference was 1.68 kg/m2 in favor of olanzapine.
That size of BMI change would be clinically relevant if it were stable and precise.
The estimate was not stable enough. The confidence interval was wide, the p value was 0.19, and the review concluded that the pooled effect did not reach statistical significance.
High Heterogeneity Made the Weight-Gain Signal Hard to Interpret
The main caution is I2 = 94%, a very high heterogeneity statistic. The included trials were not all telling the same story in the same way.
Meta-analysis can make weak evidence look stronger when readers focus only on the pooled estimate. Here, the pooled number favored olanzapine, but the spread across studies warned against treating the number as a settled treatment effect.
- Different settings: Trials mixed inpatient, outpatient, and structured program contexts.
- Different doses: Olanzapine dosing ranged across studies, with the discussion naming 2.5-10 mg as part of the variation.
- Different outcome reporting: Some trials reported weight in kilograms, some BMI change, and some lacked dispersion values needed for pooling.
- Different populations: Age ranges and anorexia nervosa subtypes were not uniform across the evidence base.
A sensitivity analysis reduced heterogeneity to 28% after excluding the most inconsistent study. Even then, the effect size did not change enough to settle the clinical uncertainty.
Psychological Symptom Findings Did Not Establish a Clear Add-On Benefit
Weight restoration is only one part of anorexia nervosa treatment. The review also summarized psychological outcomes, including obsessive eating-disorder thoughts and related symptom scales.
Those findings were mixed. One older trial reported a 54% reduction in anorexic ruminations with olanzapine compared with 9% in the control group, independent of weight gain.
Another trial reported faster target-BMI achievement and improved obsessive symptoms.
However, the larger randomized trial summarized in the review found modestly higher weight gain but no significant psychological symptom improvement compared with placebo. That split is why the paper does not support olanzapine as routine monotherapy.
- Potential niche: Selected treatment-resistant cases with prominent obsessive-compulsive symptoms may be reasonable candidates for specialist consideration.
- Not first line: The review explicitly says olanzapine should not be treated as a first-line anorexia nervosa treatment.
- Care context: Any medication effect has to sit inside nutritional rehabilitation, psychotherapy, medical monitoring, and risk management.
The difference between “may help selected patients” and “works as a standard treatment” is important. This paper supports the first possibility more than the second.
Risk of Bias and Trial Design Limited the Confidence Level
The review used the Cochrane risk-of-bias tool for randomized trials and the GRADE framework. Three studies were rated low risk of bias, while the other 4 had either some concerns or high risk.
Evidence certainty was rated moderate. That is not a dismissal, but it means the conclusion can still move when larger and cleaner trials arrive.
- Small evidence base: 7 trials is too few for confident subgroup analysis or publication-bias testing.
- Protocol variation: Treatment duration, dose, comparator, adherence, and care setting differed across trials.
- Outcome gaps: Some studies could not be pooled because they reported weight or BMI without comparable variance data.
For clinicians, the evidence supports a conservative interpretation. Olanzapine may be discussed as an adjunct in carefully selected anorexia nervosa cases, especially when obsessive or anxiety symptoms are severe, but the current randomized evidence does not justify treating it as a reliable weight-restoration solution.
Future trials need larger samples, consistent BMI and psychological outcome reporting, longer safety follow-up, and better subgroup definitions. Without that, the field will keep circling the same uncertain result: a plausible medication signal that is still too uneven to carry routine care.
Citation: DOI: 10.1186/s12888-026-08017-w. Alqurashi et al. Olanzapine effectiveness on weight gain in anorexia nervosa patients: systematic review and meta-analysis. BMC Psychiatry. 2026;26:413.
Study Design: Systematic review and random-effects meta-analysis of randomized controlled trials.
Sample Size: 7 RCTs with 152 participants; 4 trials with 91 participants entered the pooled BMI analysis.
Key Statistic: Mean BMI difference was 1.68 kg/m2 favoring olanzapine, but p = 0.19 and I2 = 94%.
Caveat: Small trials, high heterogeneity, and mixed risk-of-bias ratings keep the treatment conclusion uncertain.