TL;DR: A 2026 preprint in medRxiv found that treatment-resistant depression affected 34% of medication-exposed major-depression patients in Pakistan’s DIVERGE study, with social support and CYP2C19 metabolizer status standing out as locally important treatment-response markers.
Key Findings
- 3,677 eligible patients: The treatment-resistance analysis included adults with major depressive disorder who had medication exposure and enough adherence information for classification.
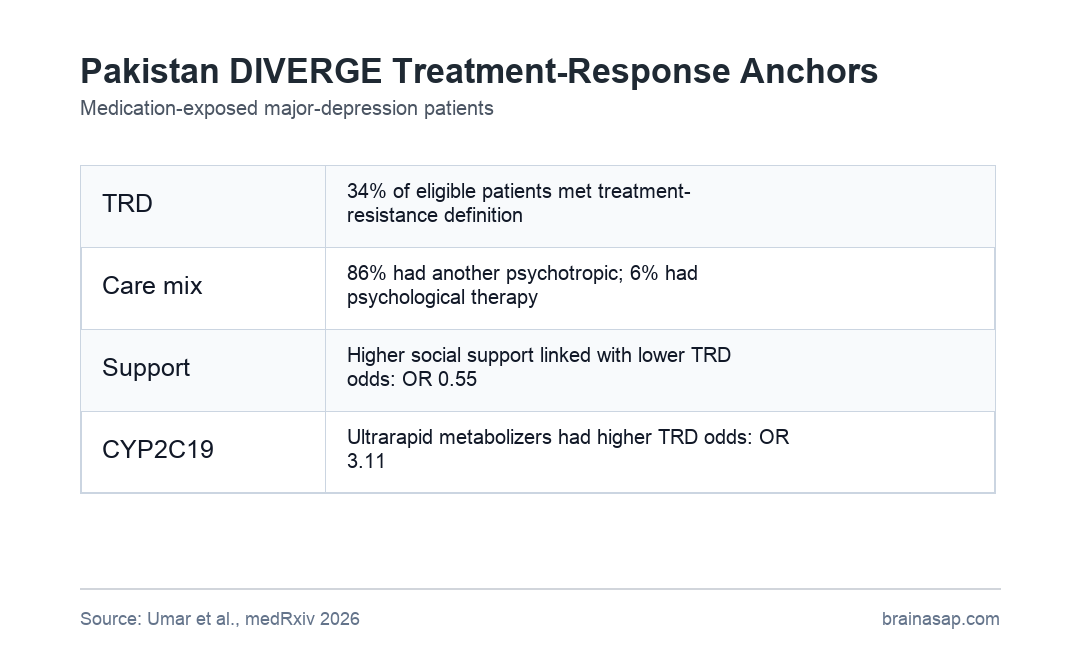
- 34% treatment resistance: 1,265 of 3,677 eligible patients met the study definition for treatment-resistant depression, with a reported 95% CI of 32% to 36%.
- 86% polypharmacy: Most medication-exposed patients were prescribed another psychotropic drug along with an antidepressant, while psychological therapy was reported in only 6%.
- Social support signal: Higher social support was associated with lower odds of treatment resistance (OR 0.55, 95% CI 0.44 to 0.69; p = 1.4 x 10^-7).
- CYP2C19 risk: In 1,085 patients with pharmacogenetic data, CYP2C19 poor metabolizers and ultrarapid metabolizers had higher treatment-resistance odds than normal metabolizers.
Source: medRxiv (2026) | Umar et al.
Treatment-resistant depression means depression symptoms have not improved enough after adequate antidepressant treatment. In this study, researchers defined it as minimal or no symptom relief after at least 12 weeks of antidepressant use with good or intermediate adherence.
The DIVERGE cohort is important because most depression-treatment evidence still comes from high-income countries. This analysis asked whether treatment resistance in Pakistan followed familiar patterns or had local features that should shape care.
DIVERGE Found 34% Treatment-Resistant Depression in Medication-Exposed Patients
Researchers recruited 8,360 adults with major depressive disorder from psychiatric care facilities across Pakistan between September 2021 and June 2025. The main treatment-resistance analysis excluded medication-naive patients and those without enough medication-history information.
That left 3,677 eligible patients. Of those, 1,265 patients were classified as treatment resistant, producing a prevalence estimate of 34%.
- Medication-naive group: 1,954 recruited patients, or 23%, had not yet used depression medication and were not eligible for the main treatment-resistance classification.
- Adherence screen: Among 6,406 patients with depression-medication history, 41% reported good adherence, 57% moderate adherence, and 2% poor adherence.
- Clinical profile: The eligible cohort was 56% female, had a mean age of 38 years, and reported a mean illness duration of 7 years.
The estimate sits in the same broad range reported in several high-income settings, but the treatment context was different. The analysis captured routine psychiatric care in a lower-income setting with heavy medication mixing and limited psychotherapy access.
Psychotropic Polypharmacy Was Common While Psychological Therapy Was Rare
The prescribing pattern was one of the clearest care-system findings. Only 14% of eligible medication-exposed patients received a single antidepressant.
The remaining 86% received at least one additional psychotropic medication. That included another antidepressant, a mood stabilizer, an antipsychotic, an anxiolytic, or a benzodiazepine.
- Combination therapy: About 29% received more than one antidepressant.
- Augmentation therapy: About 52% received an antidepressant plus a mood stabilizer or antipsychotic.
- Psychological therapy: Only 6% reported psychotherapy or another psychological treatment.
- Faith-healer contact: About 49% had visited a religious leader or faith healer for mental-health problems.
Those numbers do not prove that polypharmacy caused poor response. They show that depression care in this setting leaned heavily toward medication combinations, even though psychological treatments are part of standard depression guidelines.
Social Support Was Linked to Lower Treatment-Resistance Odds
The strongest social finding involved Oslo Social Support Scale scores, a short measure of available support. Higher social support was associated with substantially lower treatment-resistance odds.
The adjusted association was OR 0.55, with a 95% confidence interval from 0.44 to 0.69. The p-value was 1.4 x 10^-7, making it one of the most stable signals in the analysis.
- Clinical meaning: The result suggests that family and community support may influence recovery in ways that standard treatment algorithms can miss.
- Local context: Pakistan’s family structures, religious networks, and care access patterns may make support especially relevant for depression outcomes.
- Boundary: The study was observational, so social support may mark other advantages rather than directly preventing treatment resistance.
CYP2C19 Poor and Ultrarapid Metabolizers Had Higher TRD Odds
The pharmacogenetic arm used the Infinium Global Diversity Array with Enhanced PGx-8 and DRAGEN calling to infer metabolizer status. The main genes were CYP2C19 and CYP2D6, which help metabolize commonly used antidepressants.
Among 1,085 patients with CYP enzyme data, CYP2C19 stood out. Poor metabolizers had higher odds of treatment resistance than normal metabolizers, with OR 1.85 and a 95% CI of 1.11 to 3.07.
Ultrarapid CYP2C19 metabolizers showed an even larger association: OR 3.11, 95% CI 1.59 to 6.12, p = 0.0009. CYP2D6 results were not the headline signal in the extracted summary.
- Why CYP2C19 matters: Too-slow or too-fast metabolism can change drug exposure for several antidepressants.
- Precision-care angle: Pharmacogenetic testing may help identify some patients whose medication plan needs closer review.
- Missing piece: Current prescriptions were better documented than prior treatment sequences, limiting a strict two-failed-trial definition.
Suicidal Behavior and Psychotic Symptoms Marked a Higher-Risk TRD Group
Patients with treatment-resistant depression had more severe clinical markers. Psychotic symptoms were associated with higher treatment-resistance odds (OR 1.39, 95% CI 1.04 to 1.84; p = 0.02).
Suicidal behavior also tracked with treatment resistance, with OR 1.03, 95% CI 1.01 to 1.05, and p = 0.005. The effect size is smaller, but the direction matches clinical concern: harder-to-treat depression often carries greater safety risk.
The main limitation is design. Retrospective medication histories, incomplete prior-treatment sequencing, unavailable nonpsychiatric medication data, and no phenoconversion adjustment make this a risk-factor study, not a definitive treatment algorithm.
The practical result is still useful. Depression treatment in Pakistan may need better access to psychological therapy, closer review of high polypharmacy, social-support-aware care planning, and pharmacogenetic follow-up in selected patients.
Citation: DOI: 10.64898/2026.04.13.26350625. Umar et al. Understanding response to treatment in depression: Insights from the Pakistani DIVERGE study. medRxiv. 2026.
Study Design: Observational genetic epidemiology study of adults with major depressive disorder recruited from psychiatric care facilities across Pakistan.
Sample Size: 8,360 recruited MDD patients, including 3,677 medication-exposed patients eligible for treatment-resistance analysis and 1,085 with CYP enzyme data.
Key Statistic: 34% met the study definition for treatment-resistant depression; CYP2C19 ultrarapid metabolizer status was associated with OR 3.11 for treatment resistance.
Caveat: The preprint was not peer reviewed, and retrospective medication histories limited strict reconstruction of sequential antidepressant failures.