TL;DR: A 2026 study in JAMA Network Open found that a therapy built to restore reward and positive emotion outperformed a matched negative-affect therapy for adults with depression, anxiety, and severely low positive affect.
Key Findings
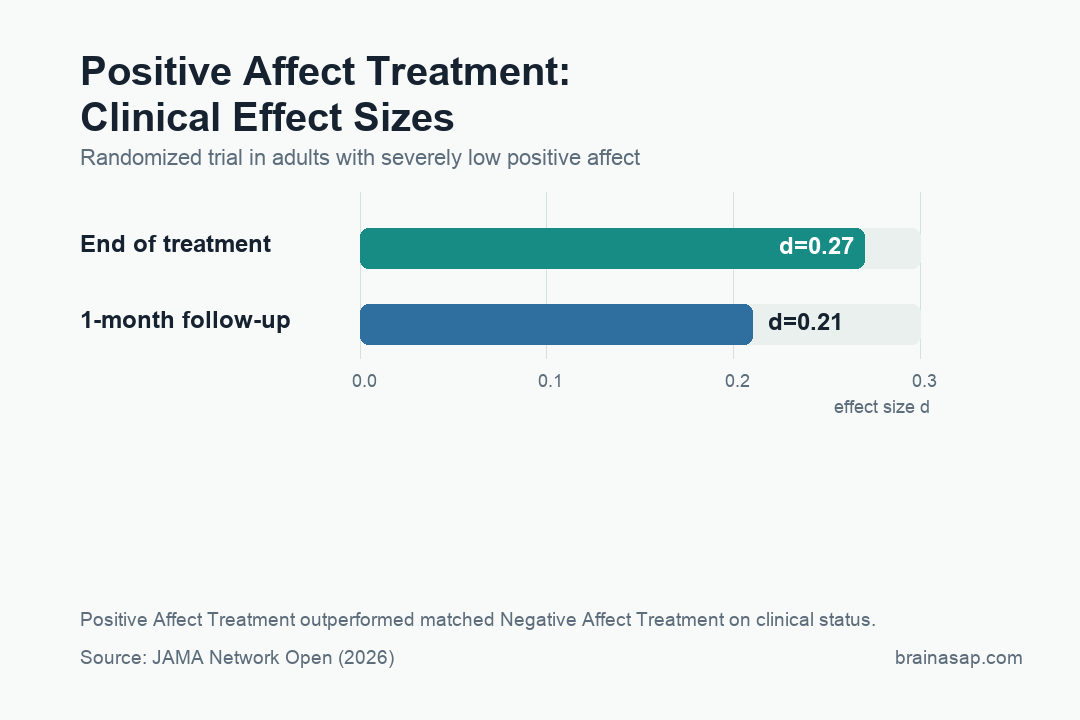
- PAT beat the matched therapy: Positive Affect Treatment improved the composite clinical-status outcome more than Negative Affect Treatment (d = 0.27; P =.02).
- Follow-up still favored PAT: At 1 month after treatment, PAT retained a smaller but significant advantage over NAT (d = 0.21; P =.04).
- 98 low-positive-affect adults randomized: Participants had severely low positive affect plus functionally impairing moderate to severe depression or anxiety.
- Fifteen weekly sessions tested the model: Both groups received individual telehealth therapy; PAT targeted reward processes, while NAT targeted negative affect and arousal.
- Self-report mechanisms showed the association: Six of seven self-reported reward and threat measures mediated clinical improvement; behavioral and physiological measures did not.
Source: JAMA Network Open (2026) | Meuret et al.
Anhedonia is one of depression’s cruelest tricks: the world does not only feel bad, it stops feeling worth reaching for.
This JAMA Network Open trial tested whether therapy should target that missing pull directly instead of working mainly through fear, distress, and negative emotion.
Anhedonia Was the Treatment Target, Not a Side Symptom
Most depression and anxiety treatments spend a lot of time reducing negative affect: fear, tension, avoidance, rumination, panic, and distress, which makes sense, but it leaves a second system under-treated.
Three details anchor the result:
- PAT beat the matched therapy: Positive Affect Treatment improved the composite clinical-status outcome more than Negative Affect Treatment (d = 0.27; P =.02)
- Follow-up still favored PAT: At 1 month after treatment, PAT retained a smaller but significant advantage over NAT (d = 0.21; P =.04)
- 98 low-positive-affect adults randomized: Participants had severely low positive affect plus functionally impairing moderate to severe depression or anxiety
A person can feel less terrified and still not feel alive, motivated, interested, or pulled toward reward.
Positive Affect Treatment, or PAT, was built around that gap.
Its modules targeted reward anticipation and motivation, reward attainment, and reward learning.
The comparison therapy, NAT, was not a weak control; it was a structurally similar treatment aimed at reducing negative affect and arousal.
The comparison isolates the active clinical target.
This was not therapy versus nothing.
It was a test of which emotional system should be pushed when patients enter treatment with severely low positive affect.
Fifteen Telehealth Sessions Put Reward Against Threat
The trial randomized 98 adults at academic outpatient centers in Los Angeles and Dallas. Participants had severely low positive affect plus moderate to severe, functionally impairing depression or anxiety.
Both groups received 15 weekly one-on-one manualized sessions by telehealth. The treatments shared structure but differed in target:
- PAT: trained reward anticipation, reward experience, and reward learning so patients could rebuild the machinery of wanting, enjoying, and updating from positive outcomes.
- NAT: focused on reducing negative affect and arousal, a more familiar therapeutic target in depression and anxiety care.
- Shared structure: both treatments used 15 weekly telehealth sessions, which made the target difference easier to interpret.
The primary clinical-status composite combined self-reported positive affect, interviewer-rated anhedonia, and self-reported depression and anxiety. That mix is important because the trial was not only asking whether mood improved.
It was asking whether the reward system moved with clinical recovery. The main result was modest in size but clean in direction.
Clinical status improved more with PAT than NAT, with an effect size of d = 0.27.
At the 1-month follow-up, the PAT advantage remained significant at d = 0.21.
The advantage was driven mainly by greater reductions in depression and anxiety symptoms, rather than a uniquely larger jump in positive affect or interviewer-rated anhedonia.
That is a helpful surprise.
A reward-focused treatment did not only make people report more positive emotion; it improved broader clinical status.
Reward anticipation and motivation improved over time, as did reward attainment.
Those effects were not exclusive to PAT, which complicates the neat interpretation.
Both therapies moved reward and threat processes, but the therapy explicitly built around reward still produced the better clinical-status trajectory.
The Mechanism Was Psychological Before It Was Physiological
The mediation result is the most revealing part of the trial. Of seven self-reported reward and threat measures, six mediated clinical improvement. None of the behavioral or physiological target measures did.
That does not make the result weak.
It tells us where the readout was strongest: in patients’ reported reward drive, reward anticipation, reward consumption, threat sensitivity, and related psychological processes.
Therapy may first change how reward and threat are represented and pursued in daily life before lab physiology cleanly registers the shift.
The paper also prevents a simplistic “reward therapy only works through reward” story. Threat-related self-report measures helped explain improvement too.
Depression and anxiety do not divide neatly into pleasure on one side and fear on the other. Treatment that revives reward can also change how threatening the world feels.
A Small Trial Still Changes the Therapy test
This was a 98-person randomized trial, not a definitive practice guideline.
The effect sizes were small, and the strongest mediators were self-reported, which means they share method overlap with clinical symptom reports.
The follow-up was also short.
But the study asks the right clinical test.
If a patient is depressed or anxious and also severely low in positive affect, should treatment mainly reduce bad feelings, or should it actively rebuild the ability to anticipate, seek, and learn from reward?
This trial points toward the second answer.
It does not replace CBT, medication, exposure therapy, or other evidence-based care.
It argues that reward restoration deserves a front-row seat, especially for patients whose core problem is not only feeling terrible but feeling unable to want.
The telehealth format also matters.
A reward-focused therapy that can be delivered remotely is easier to imagine scaling than a highly specialized laboratory intervention.
The open test is whether clinicians outside the trial can deliver PAT with the same fidelity and whether the advantage survives longer follow-up.
Future studies should also test who benefits most.
Low positive affect can show up in major depression, anxiety disorders, trauma-related disorders, substance use recovery, and chronic illness.
PAT may not be the right answer for all of them, but the trial gives a cleaner way to match treatment target to symptom profile.
That matching test is where psychotherapy research often gets stuck.
Average effects can look modest because the treatment is diluted across patients whose dominant problem is different.
A low-positive-affect entry criterion is one way to make the trial more biologically and clinically coherent.
It also gives future trials a clearer endpoint: not just fewer symptoms, but restored approach, interest, and reward learning.
Depression Recovery Needs More Than Symptom Removal
The deeper implication is about what recovery means.
A treatment can reduce distress and still leave a person with a life that feels flat.
PAT takes the opposite angle: rebuild reward learning so future experience becomes worth pursuing.
The distinction is important for relapse and suicidality, because low positive affect and anhedonia are not cosmetic symptoms.
They influence motivation, social connection, and whether a patient can imagine tomorrow as something other than endurance.
Brain ASAP’s read is straightforward: this is not a flashy treatment claim, but it is a smart one.
The trial moves psychotherapy closer to the specific circuitry of depression and anxiety, where reward, threat, and motivation are not abstractions.
They are the levers that decide whether treatment gives someone less pain, or a life that starts pulling again.
Citation: DOI: 10.1001/jamanetworkopen.2026.7403. Meuret et al. Positive Affect Treatment for Depression, Anxiety, and Low Positive Affect: A Randomized Clinical Trial. JAMA Network Open. 2026;9(4):e267403
Study Design: Assessor-blinded, multisite, 2-arm randomized clinical superiority trial.
Sample/Model: 98 treatment-seeking adults with severely low positive affect plus moderate to severe depression or anxiety.
Key Statistic: PAT improved clinical status more than NAT (d = 0.27; P =.02), with a significant advantage still present 1 month after treatment.
Caveat: Single-study evidence; interpret with the source design and sample.