TL;DR: A 2026 study in European Archives of Psychiatry and Clinical Neuroscience linked sustained quetiapine treatment with better high-working-memory cognitive performance in schizophrenia spectrum disorder, but the genetic tests did not support the proposed remyelination-moderation mechanism.
Key Findings
- 166 matched pairs: The extended PsyCourse analysis included 166 quetiapine-treated schizophrenia-spectrum patients and 166 age- and sex-matched patients not receiving quetiapine.
- 106 sustained pairs: The main longitudinal comparison focused on 106 patients receiving quetiapine at two visits about 6 months apart and 106 matched non-quetiapine patients.
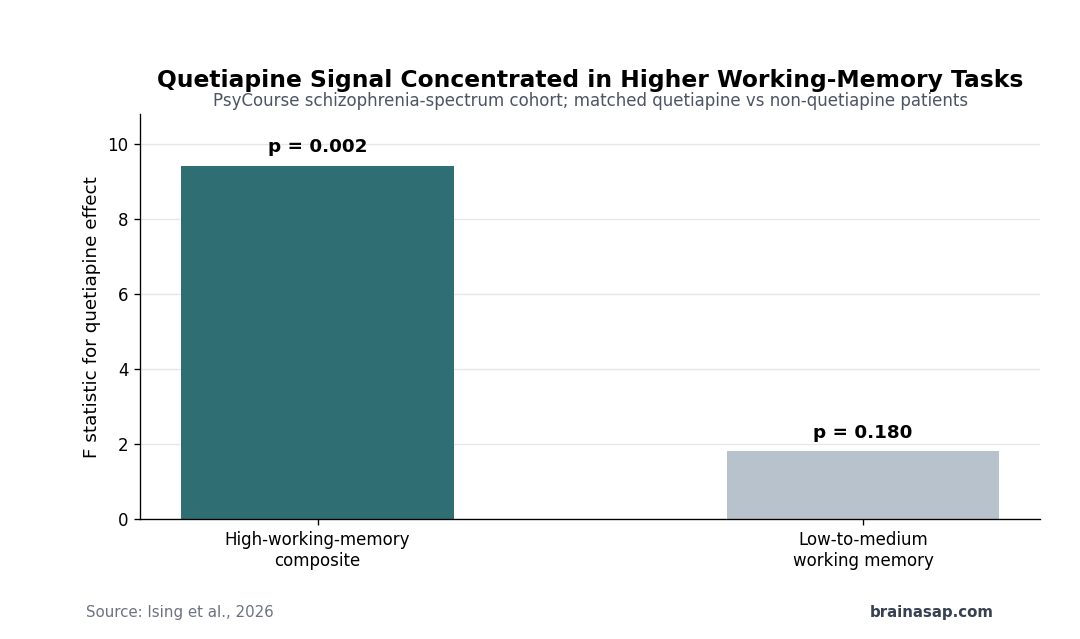
- High-memory advantage: Quetiapine status predicted the high-working-memory composite score, with F = 9.42 and p = 0.002 in the main composite analysis.
- Low-memory null: Low-to-medium working-memory tests did not show the same quetiapine effect, with F = 1.81 and p = 0.180 for the LowWM composite.
- No genetic moderation: Polygenic proxy scores for hippocampal volumes, white-matter integrity, and oligodendrocyte-related schizophrenia risk did not significantly moderate the quetiapine-cognition association.
Source: European Archives of Psychiatry and Clinical Neuroscience (2026) | Ising et al.
Quetiapine is usually discussed as an antipsychotic for symptoms such as delusions, hallucinations, mood instability, or sleep disruption. This study asked a narrower question: whether sustained quetiapine use in schizophrenia spectrum disorder was associated with better cognition on tasks that heavily tax working memory.
The researchers also tested a proposed biological explanation. Prior lab and imaging work has connected schizophrenia-related cognitive impairment with oligodendrocyte and myelin abnormalities, so the team asked whether genetic proxies for hippocampal volume, white-matter integrity, or oligodendrocyte-related risk changed the apparent quetiapine effect.
Quetiapine Was Tested Against Matched Schizophrenia Controls
The analysis used the prospective PsyCourse study, a longitudinal cohort of people with schizophrenia spectrum disorders and related conditions. For the main sustained-treatment analysis, researchers compared 106 quetiapine-treated patients with 106 matched patients who were not receiving quetiapine.
Matching was based on age and sex, and visits were separated by about 6 months. The broader sensitivity analysis added patients with one quetiapine visit, producing an extended comparison of 166 quetiapine patients and 166 non-quetiapine patients.
- Medication contrast: The non-quetiapine group was not medication-free; most patients were receiving other second-generation antipsychotics, making the comparison more specific than treated versus untreated illness.
- Mean dose: In the sustained-treatment sample, reported quetiapine dose averaged about 543 mg/day, with substantial variation across patients.
- Genetic layer: Polygenic scores were calculated for brain-volume traits, diffusion-tensor white-matter measures, and cell-type-specific schizophrenia risk.
This was still an observational medication analysis, not a randomized quetiapine trial. Clinical reasons for choosing quetiapine can also track illness profile, sedation burden, symptom pattern, and treatment history.
High-Working-Memory Tests Showed the Quetiapine Signal
The cognitive battery was split by working-memory demand. Lower-demand tests included Trail Making Test A and digit span forward, while the high-working-memory group included Trail Making Test B, digit span backward, Digit Symbol Substitution Test, and verbal learning measures.
Quetiapine-treated patients performed better on the higher-demand composite. The main high-working-memory comparison was significant at F = 9.42 with p = 0.002, and the authors described the effect as near a medium size.
- Task specificity: The effect concentrated in tests requiring manipulation, sequencing, or consolidation of information rather than simpler attention or processing tasks.
- TMT-B nuance: Trail Making Test B was not significant across both visits in the parametric model, but visit-2 performance favored the quetiapine group.
- DSST nuance: The Digit Symbol Substitution Test showed a weaker pattern, becoming significant only when visit 2 was considered separately.
- LowWM contrast: The low-to-medium working-memory composite did not show a quetiapine effect, with p = 0.180.
The result therefore should not be generalized to every cognitive measure. It points to a selective association with tasks that place heavier demands on working memory.
Lower Quetiapine Dose Was Linked to Better High-Memory Scores
Among quetiapine-treated patients, higher dose did not explain better cognition. The dose analysis showed a negative association between quetiapine dose and high-working-memory performance, with r = -0.26 and p = 0.007.
Researchers then looked at a lower-dose subgroup. Patients receiving 300 mg/day or less showed stronger high-working-memory performance than their matched non-quetiapine comparison group.
- Lower-dose subgroup: The analysis compared 29 quetiapine-treated patients at 300 mg/day or below with matched non-quetiapine patients.
- HighWM score: The lower-dose quetiapine subgroup had a mean high-working-memory score of 52.4, compared with 45.6 in matched controls.
- Clinical interpretation: Higher quetiapine doses may carry sedation or illness-severity confounding, so dose findings should not be read as a simple dosing recommendation.
This dose pattern is useful mainly as a caution. A medication-cognition association can be shaped by who receives the drug, why the dose is chosen, and what else is happening clinically.
Polygenic Scores Did Not Support the Remyelination Hypothesis
The mechanistic hypothesis was that quetiapine might improve cognition partly through remyelination or oligodendrocyte-related biology. If that were true, genetic proxies for hippocampal volume, white-matter integrity, or oligodendrocyte-related schizophrenia risk might have changed the size of the quetiapine association.
That moderation test was negative. Across the brain-volume, white-matter, and cell-type-specific analyses, researchers did not find significant interactions showing that these polygenic scores modified the quetiapine effect on high-working-memory performance.
- Brain-volume scores: Polygenic proxy scores for hippocampus-related brain volumes did not moderate the quetiapine association.
- White-matter scores: Diffusion-tensor imaging proxy scores also failed to explain who appeared to benefit cognitively.
- Oligodendrocyte-risk scores: Cell-type-specific risk scores did not support the idea that oligodendrocyte-related schizophrenia risk shaped the quetiapine-cognition link.
One separate genetic result did appear: lower schizophrenia-risk loading in oligodendrocyte-related genes was associated with better cognitive performance independent of quetiapine. That finding fits the broader oligodendrocyte question, but it is not evidence that quetiapine worked through genetic differences in remyelination capacity.
The Cognitive Finding Needs Randomized Confirmation
The cohort result is specific. Sustained quetiapine use was associated with better performance on cognitively demanding working-memory tasks in schizophrenia spectrum disorder, while the proposed polygenic-remyelination moderator was not supported.
The strongest limitation is the nonrandomized design. Quetiapine choice, dose, side effects, sleep, symptom profile, and other medications could all influence cognitive testing, even when groups are matched and regression models adjust for measured covariates.
For clinicians and researchers, the study is best treated as a targeted cohort result rather than a treatment rule. It supports asking whether quetiapine has cognition-relevant effects in some schizophrenia patients, but it does not prove that switching to quetiapine will improve working memory.
Citation: DOI: 10.1007/s00406-026-02309-8. Ising et al. Effects of quetiapine on cognitive functioning in schizophrenia: evidence for the remyelination hypothesis? European Archives of Psychiatry and Clinical Neuroscience. 2026.
Study Design: Prospective observational PsyCourse cohort analysis comparing quetiapine-treated schizophrenia-spectrum patients with matched non-quetiapine patients.
Sample Size: Main sustained-treatment analysis used 106 matched pairs; extended analysis used 166 quetiapine patients and 166 matched controls.
Key Statistic: Quetiapine status predicted the high-working-memory composite (F = 9.42, p = 0.002), while the low-to-medium working-memory composite was not significant (p = 0.180).
Caveat: Medication exposure was not randomized, so the cognitive association may still reflect patient selection, dose choice, illness differences, or other treatment factors.