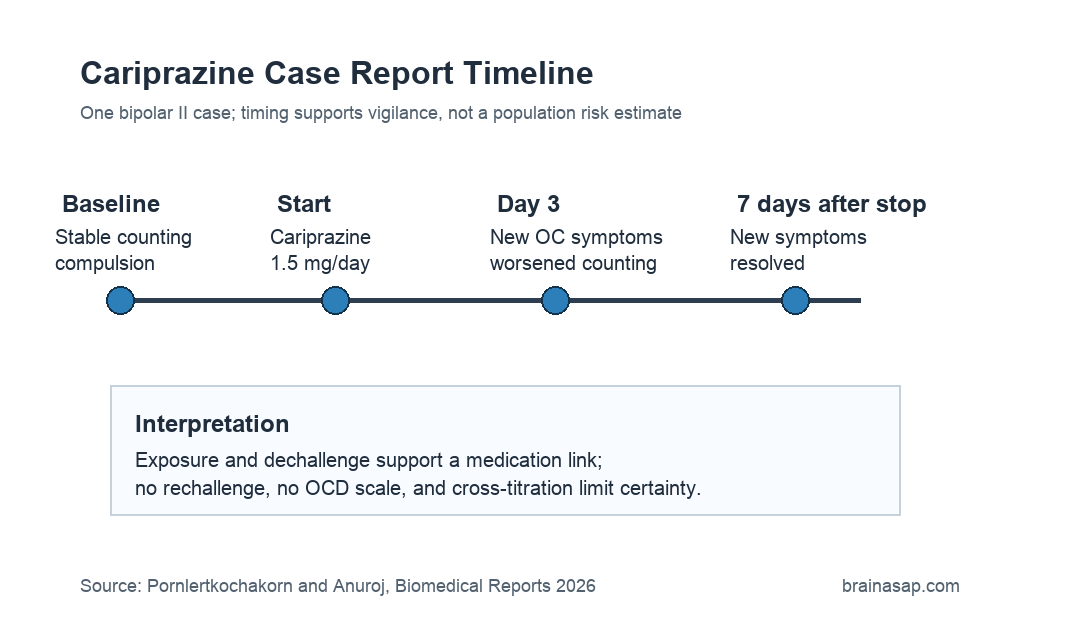
TL;DR: A 2026 case study in Biomedical Reports described a 28-year-old woman with bipolar II disorder whose stable subclinical counting compulsion worsened and expanded into new obsessive-compulsive symptoms within 3 days of starting cariprazine, then returned near baseline within 7 days after the drug was stopped.
Key Findings
- Single case report: The source described one 28-year-old Thai woman with bipolar II disorder and adolescent-onset subclinical counting compulsion.
- 1.5 mg/day cariprazine: Cariprazine was started during a switch away from aripiprazole after akathisia limited aripiprazole dose escalation.
- 3-day onset: After 3 days on cariprazine, new intrusive religious-profane thoughts, catastrophic family-accident images, worsened counting, and self-pinching undoing behavior emerged.
- 7-day resolution: The new obsessive-compulsive symptom clusters resolved within 7 days after cariprazine discontinuation, while counting returned to baseline subclinical severity.
- Causality remained suggestive: No rechallenge was performed, no standardized Yale-Brown Obsessive Compulsive Scale rating was used, and medication cross-titration limited certainty.
Source: Biomedical Reports (2026) | Pornlertkochakorn and Anuroj
Cariprazine is an atypical antipsychotic used in schizophrenia and bipolar disorder. This report does not show that cariprazine commonly causes obsessive-compulsive symptoms, but it gives clinicians a detailed timeline for one possible adverse psychiatric reaction.
The patient already had a mild counting compulsion that began in adolescence and stayed stable during the months before cariprazine. The notable change was not simply the presence of obsessive-compulsive symptoms, but the abrupt shift from stable subclinical counting to distressing new symptom clusters after the medication switch.
Cariprazine Was Started During a Bipolar II Medication Switch
The patient was a 28-year-old woman with bipolar II disorder. Before the index event, she had been treated with aripiprazole, sertraline, clonazepam, and a brief lamotrigine trial that stopped after an allergic skin reaction.
Aripiprazole helped hypomanic symptoms but caused akathisia at 2.5-5 mg/day, which limited further titration. The patient declined quetiapine because of metabolic concerns, so clinicians selected cariprazine 1.5 mg/day.
- Premorbid symptom: a stable counting compulsion present since adolescence.
- Switch context: aripiprazole was reduced from 5 mg/day to 2.5 mg/day and then stopped.
- New medication: cariprazine was introduced at 1.5 mg/day on the same day the aripiprazole dose was reduced.
That cross-titration is central to the interpretation. The timing points toward cariprazine exposure, but the overlapping change in aripiprazole means the case cannot isolate one pharmacological cause with certainty.
New Obsessive-Compulsive Symptoms Emerged After 3 Days
After 3 days on cariprazine, the patient reported two new forms of obsessive-compulsive symptoms. One involved intrusive thoughts about desecrating or uttering profanities toward religious objects, and another involved recurrent fear-provoking images of catastrophic accidents affecting family members.
The existing counting compulsion also became more frequent and intense. A new undoing compulsion appeared, described as self-pinching when the counting was not performed properly.
- Intrusive religious thoughts: unwanted thoughts involving religious objects and profanities.
- Catastrophic mental images: fear-provoking accident images involving family members without a matching traumatic trigger.
- Counting escalation: a previously benign compulsion became distressing and functionally impairing.
- Undoing behavior: self-pinching appeared when counting felt improperly completed.
Clinical assessment did not identify recent psychosocial stressors, infection symptoms, immune-mediated features, concurrent medical illness, other new psychiatric symptoms, or other new medications. Insight into the irrationality of the obsessive-compulsive phenomena was preserved.
Symptoms Resolved Within 7 Days After Cariprazine Stopped
At the index visit, the treatment plan changed back to aripiprazole 5 mg/day, and sertraline was restarted at 25 mg/day for persistent depressive symptoms. Within 7 days after stopping cariprazine, the two newly emerged obsessive-compulsive symptom clusters had fully resolved.
The counting compulsion returned to its baseline subclinical severity. At follow-up visits up to 1.5 months later, the counting compulsion remained at baseline.
- Dechallenge pattern: symptoms improved after the suspected medication was stopped.
- Rechallenge absent: cariprazine was not restarted because the patient refused rechallenge.
- Sertraline timing: the authors considered a full sertraline effect unlikely because improvement occurred within 7 days at a low dose.
This timeline is the strongest part of the case report. It does not prove causality, but it gives a plausible temporal association: onset after exposure, resolution after discontinuation, and no obvious acute stressor identified at symptom onset.
Dopamine and Serotonin Mechanisms Remained Hypothetical
Cariprazine acts as a partial agonist at dopamine D2 and D3 receptors and serotonin 5-HT1A receptors, and as an antagonist at serotonin 5-HT2A and 5-HT2B receptors. The authors discussed serotonergic and dopaminergic systems because obsessive-compulsive symptoms can involve cortico-striato-thalamo-cortical circuitry.
The report also noted that obsessive-compulsive symptoms have been described with other second-generation antipsychotics, especially clozapine, and less often with olanzapine, risperidone, or quetiapine. Cariprazine-specific reports remain limited.
- D3 affinity: cariprazine has high affinity for dopamine D3 receptors.
- Serotonin activity: the drug also affects several serotonin receptor systems.
- Circuit context: obsessive-compulsive symptoms are linked to cortico-striato-thalamo-cortical loops.
Those mechanisms are plausible context, not direct evidence from this patient. The case did not include neuroimaging, receptor-level testing, or a controlled medication challenge.
The Case Supports Monitoring, Not a General Risk Estimate
The main clinical implication is targeted monitoring during the first week of cariprazine treatment, especially in patients with pre-existing subclinical obsessive-compulsive symptoms. The authors specifically emphasized vulnerability in people whose mild symptoms may not have been formally evaluated.
The limitations are substantial. Symptom assessment relied on clinical interview and patient report rather than the Yale-Brown Obsessive Compulsive Scale or a structured interview.
There was no drug washout, no rechallenge, and a short cross-titration period.
- Single patient: the report cannot estimate how often this reaction occurs.
- Medication overlap: aripiprazole tapering and clonazepam exposure could not be fully excluded as contributors.
- Baseline vulnerability: the patient already had adolescent-onset subclinical counting compulsion.
A careful conclusion is that cariprazine may have exacerbated pre-existing obsessive-compulsive vulnerability in this patient. It is a reason to ask about obsessive-compulsive symptoms before and soon after treatment changes, not a reason to assume the same reaction will occur in most patients.
Citation: DOI: 10.3892/br.2026.2168. Pornlertkochakorn and Anuroj. Cariprazine-induced obsessive-compulsive symptoms in a patient with bipolar II disorder: A case report. Biomedical Reports. 2026;25:95.
Study Design: Single-patient adverse-event case report with literature discussion.
Sample Size: One 28-year-old woman with bipolar II disorder and premorbid subclinical counting compulsion.
Key Statistic: New obsessive-compulsive symptoms emerged after 3 days of cariprazine and resolved within 7 days after discontinuation.
Caveat: No rechallenge, no standardized obsessive-compulsive severity scale, and medication cross-titration limited causal certainty.