TL;DR: A 2026 randomized trial in Physiotherapy Research International found that adding active 5 Hz repetitive transcranial magnetic stimulation (rTMS) over the dorsolateral prefrontal cortex to dual-task stroke rehabilitation produced larger gains in Timed Up-and-Go performance, balance confidence, and cognitive screening than sham stimulation plus the same training.
Key Findings
- Small randomized trial: The study enrolled 30 people with subacute stroke, with 15 assigned to active rTMS and 15 to sham stimulation.
- Two-week dose: Participants received 10 weekday sessions of stimulation over the ipsilesional dorsolateral prefrontal cortex before dual-task exercise.
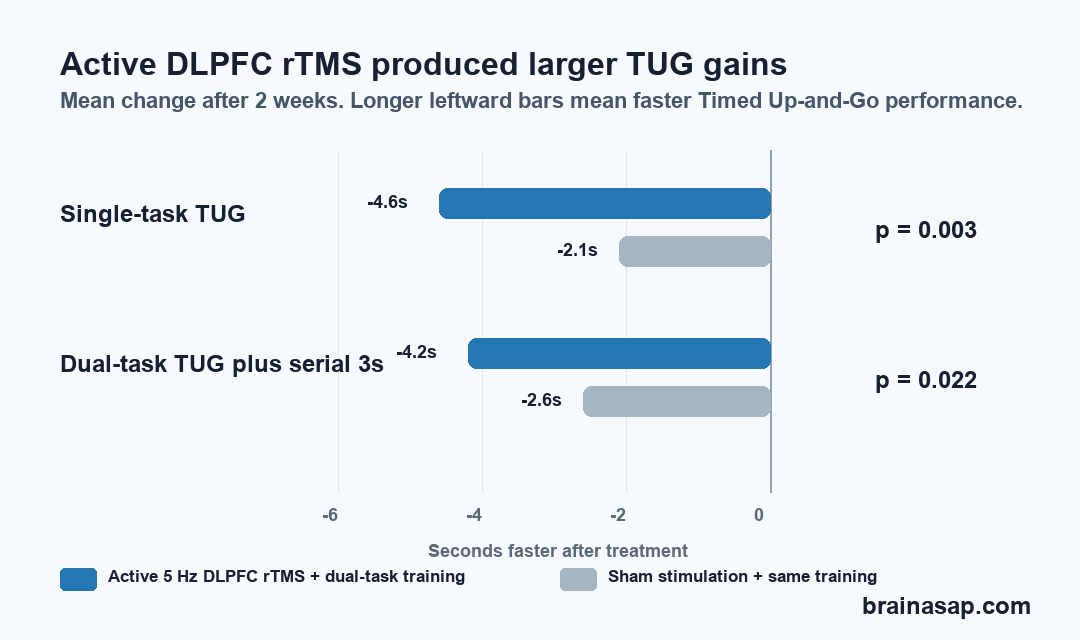
- Timed Up-and-Go improved: Active rTMS reduced single-task TUG time by 4.6 seconds versus 2.1 seconds in controls, with a significant group-by-time effect.
- Dual-task TUG also improved: During a walking-plus-serial-subtraction condition, TUG time improved by 4.2 seconds with active rTMS versus 2.6 seconds with sham.
- Main limit: The trial was small, short, and limited to mild-to-moderate motor and cognitive impairment after subacute stroke.
Source: Physiotherapy Research International (2026) | Yang et al.
Active DLPFC rTMS Was Added Before Dual-Task Training
Walking recovery after stroke is not only about moving faster in a straight line. Everyday mobility also depends on attention, balance, turning, and the ability to keep moving while the environment demands another task.
Dual-task training targets that problem directly. It asks a patient to move while also doing a cognitive task, such as counting or naming words.
Community walking rarely happens in a quiet laboratory. A person may need to walk while talking, avoiding obstacles, remembering directions, or carrying something.
After stroke, that split-attention demand can expose mobility problems that a standard single-task walk may miss.
The researchers enrolled 30 subacute stroke patients with a mean age of 59.2 years. The average time since stroke onset was about 104 days.
Most participants used an outdoor walking aid. The sample was split evenly between active stimulation and sham stimulation.
- Active group: 5 Hz rTMS was applied over the dorsolateral prefrontal cortex on the side of the stroke lesion.
- Control group: Sham stimulation was delivered before the same dual-task exercise program.
- Training schedule: Sessions were planned for 5 days per week for 2 weeks, with dual-task training after stimulation.
The stimulation dose was 1200 pulses per session at 90% of resting motor threshold. Attendance was high: participants completed an average of 9.2 of 10 sessions.
Timed Up-and-Go Gains Were Larger With Active Stimulation
The clearest mobility result came from the Timed Up-and-Go (TUG) test, a common measure in which a person stands, walks, turns, returns, and sits. Faster completion usually reflects better functional mobility and balance.
Under the single-task condition, the active rTMS group improved from 21.1 seconds to 16.5 seconds. The sham group improved from 21.3 seconds to 19.2 seconds.
The between-group difference was statistically significant, with a group-by-time result of p = 0.003.
Under the dual-task serial-subtraction condition, the active group improved from 23.6 seconds to 19.4 seconds. The sham group improved from 23.4 seconds to 20.8 seconds.
The group-by-time comparison was also significant, with p = 0.022.
- Single-task TUG: active rTMS improved by 4.6 seconds, compared with 2.1 seconds in the sham group.
- Dual-task TUG: active rTMS improved by 4.2 seconds, compared with 2.6 seconds in the sham group.
- Walking speed: both groups improved, but the between-group difference was not the strongest signal.
Step length on the affected side also favored the active group in the single-task walk and in the dual-task serial-subtraction condition.
Cadence, or steps per minute, was less consistent and did not show significant dual-task group differences.
Cognition and Balance Scores Also Favored rTMS
The trial was not only about gait. Researchers also tested cognitive and balance outcomes, including the Montreal Cognitive Assessment (MoCA), a broad cognitive screening test, and the Mini-BESTest, a balance evaluation.
The active rTMS group had better gains in MoCA, Mini-BESTest, and Activities-specific Balance Confidence scores than the control group.
This fits the study target: the dorsolateral prefrontal cortex is involved in attention and executive control. Both are relevant when walking and thinking at the same time.
The cognitive dual-task findings were narrower. Better cognitive-task gain appeared mainly when verbal fluency was paired with the 10-meter walk.
The study did not show a uniform advantage across every gait and cognition pairing.
- Most consistent mobility finding: TUG time improved more with active rTMS.
- Broader functional finding: balance and confidence scores also improved more in the active group.
- Less consistent finding: cadence and some dual-task cognitive outcomes did not clearly separate the groups.
Small Stroke Trial Needs Larger Follow-Up
No serious or mild adverse events, including headache or scalp discomfort, were reported during the 2-week intervention. This supports feasibility, but it does not prove long-term safety or durability.
The main limitation is scale. This was a 30-person randomized trial, not a large multicenter rehabilitation study.
The treatment window was short, and follow-up was immediate. Participants also had mild-to-moderate impairment rather than the full range of stroke severity.
The trial also combined two active ideas: brain stimulation and dual-task training. Because both groups received dual-task training, the comparison isolates the added value of active stimulation over sham.
It does not answer whether rTMS alone would help, or whether the same effect would hold with different stimulation targets, longer treatment, or home-based training.
For clinicians and patients, the safest reading is cautious. DLPFC rTMS before dual-task physiotherapy may help some subacute stroke patients practice mobility under real-world attention demands.
The next test is whether larger trials can replicate the TUG, balance, and cognitive-screening gains and show that they persist after rehabilitation ends.
Citation: DOI: 10.1002/pri.70259. Yang et al. rTMS Over Dorsolateral Prefrontal Cortex Augments Dual-Task Training for Mobility, Balance and Cognition in Sub-Acute Stroke: A Randomized Controlled Trial. Physiotherapy Research International. 2026;31:e70259.
Study Design: Randomized controlled trial comparing active rTMS plus dual-task training with sham stimulation plus dual-task training.
Sample Size: 30 subacute stroke patients, with 15 participants in each group.
Key Statistic: Single-task TUG improved by 4.6 seconds with active rTMS versus 2.1 seconds with sham; dual-task TUG with serial subtraction improved by 4.2 versus 2.6 seconds.
Caveat: The study was small, short, and limited to patients with mild-to-moderate motor and cognitive impairment.