TL;DR: A 2026 study in Biological Psychiatry: Global Open Science linked serious physical injury to recurrent major depression and found that injury-related DNA methylation patterns differed by depression status, with oxytocin, GABA, and synaptic-plasticity pathways standing out.
Key Findings
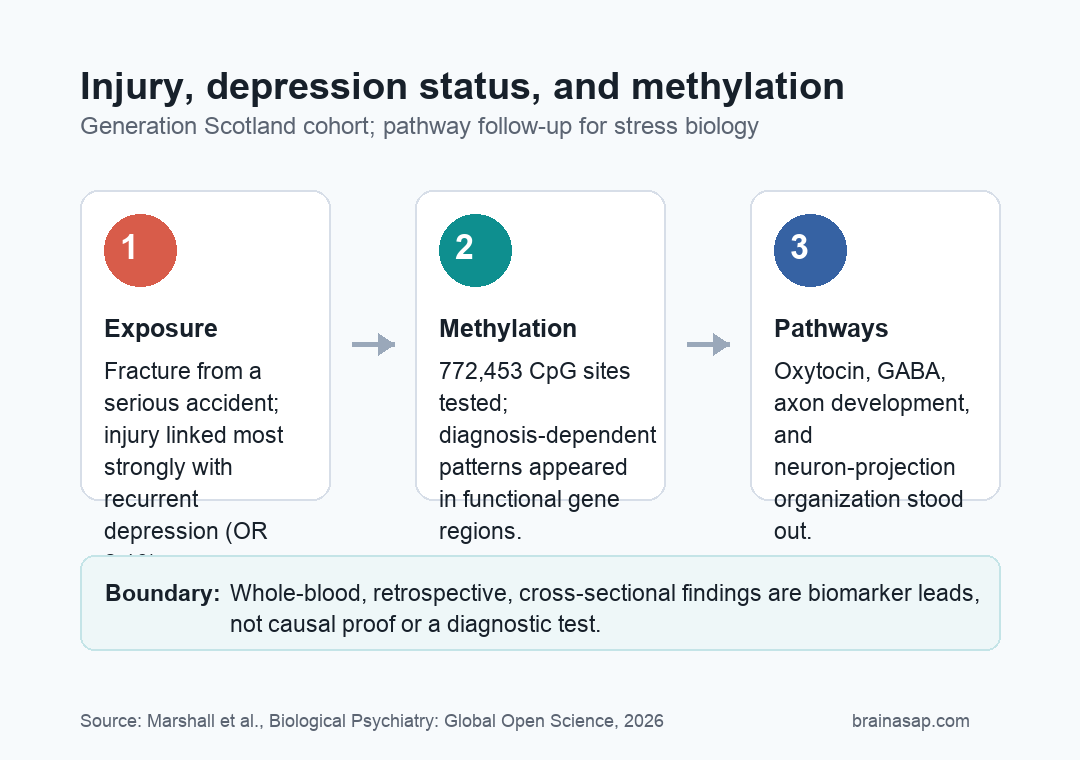
- Large cohort anchor: researchers analyzed 4,308 Generation Scotland participants with or without a reported fracture from a serious accident.
- Physical injury tracked with depression: traumatic injury was associated with lifetime depression, especially recurrent major depressive disorder.
- Recurrent depression showed the stronger association: the recurrent MDD association had an odds ratio of 2.10, compared with 1.67 for lifetime depression overall.
- Methylation patterns differed by diagnosis: injury-related DNA methylation signals varied between controls and people with recurrent depression.
- Oxytocin and synaptic pathways stood out: downstream analyses pointed to oxytocin signaling, GABAergic signaling, axon development, and neuron-projection organization.
Physical injury can be followed by depression, posttraumatic stress symptoms, or no lasting psychiatric diagnosis at all. That mixed outcome makes trauma biology difficult to interpret.
The injury may matter, but the same event does not leave the same mental-health trace in every person.
Researchers used a large Scottish cohort to ask a narrower question: when people report a serious accident that caused a fracture, do their DNA methylation patterns differ depending on whether they also have depression?
DNA methylation is a chemical mark on DNA that can influence gene activity without changing the genetic code itself.
The study is not saying that a blood methylation test can diagnose trauma-related depression. It suggests that injury exposure, recurrent depression, and stress-related pathways may overlap in measurable ways.
Generation Scotland Data Linked Injury With Recurrent Depression
The discovery analysis used 4,308 Generation Scotland participants. Researchers separated people by reported traumatic injury and depression status, then compared controls, people with single or recurrent major depression, and people with recurrent major depressive disorder.
The injury measure was specific: a traumatic incident that caused a bone fracture. That definition does not capture every trauma exposure, but it gives the analysis a concrete physical-injury anchor rather than a broad life-stress label.
The first result was clinical rather than molecular. Traumatic injury was associated with a lifetime diagnosis of depression, with an odds ratio of 1.67.
The association was stronger for recurrent major depression, with an odds ratio of 2.10.
- Discovery cohort: 4,308 participants were analyzed for injury, depression status, and methylation patterns.
- Independent follow-up sample: 2,759 participants were used for pathway-level validation against trauma, PTSD, and major depression outcomes.
- Recurrent depression focus: the strongest clinical association appeared in people with recurrent major depressive disorder, not single-episode depression.
Researchers also reported higher scores on mood-disorder and schizotypal-personality measures among people with traumatic injury, especially the disorganized factor. This finding cannot establish that the injury caused those symptoms.
The point is narrower: the exposed group carried a broader psychiatric-symptom pattern that needed to be considered alongside methylation.
Methylation Was Tested Across More Than 770,000 CpG Sites
The molecular analysis looked at DNA methylation at 772,453 CpG sites. CpG sites are locations in the genome where methylation is commonly measured.
The team used methylome-wide association and methylome-wide environment interaction analyses to test whether injury-related methylation differed by depression diagnosis.
One important pattern involved functional sequence regions. Among CpG sites showing nominally significant injury-by-diagnosis differences between controls and recurrent-depression participants, the researchers reported enrichment patterns tied to first exons, 3-prime untranslated regions, and exon boundaries.
Those locations matter because methylation near gene boundaries can relate to gene expression or splicing.
The standout pathway result was not a single “depression gene.” It was a set of biological systems that already make sense for stress biology:
- Oxytocin signaling: relevant to social behavior, stress response, and candidate trauma-related treatment biology.
- GABAergic signaling: part of inhibitory neural signaling and stress-circuit regulation.
- Synaptic plasticity: the brain’s ability to change connection strength, including during fear learning and extinction.
- Neuron-projection organization: pathways related to how neural connections and axons are shaped.
That pathway-level framing is important. Methylation studies can produce long lists of sites, many of which are hard to interpret alone.
Grouping findings by pathway helps ask whether the biology points toward stress-response systems instead of isolated statistical hits.
Brain-Region Mapping Pointed Toward Limbic Stress Systems
The researchers also asked whether methylation differences mapped onto gene-expression patterns in brain regions. Differential methylation in recurrent depression was associated with gene expression in the limbic lobes and supraoptic nuclei.
That does not prove that blood methylation directly measured brain methylation. The methylation samples came from whole blood, not brain tissue.
The brain-region mapping still gives a biological clue: the implicated expression patterns sit near systems involved in stress response, fear memory, social behavior, and emotion regulation.
The downstream validation work used pathway-specific methylation risk scores, polygenic risk scores, and SNP heritability analyses.
Put more directly, the team asked whether the pathways highlighted by methylation also carried genetic or methylation-based associations with trauma exposure, PTSD, or major depression.
- Methylation risk scores tested whether pathway-level methylation patterns related to psychiatric outcomes in another sample.
- Polygenic risk scores tested whether common genetic variation in those pathways related to depression or trauma-linked phenotypes.
- SNP heritability tested whether pathway-specific genetic variation carried more evidence than expected.
Across those analyses, pathways involving axon development and neuron projection organization appeared for recurrent depression and PTSD-related findings.
The result fits a broad stress-memory interpretation: after serious injury, vulnerability may depend partly on how stress biology intersects with neural-plasticity systems.
Whole-Blood Methylation Cannot Prove Trauma Causality
This was a cohort and pathway study suggesting that traumatic physical injury and recurrent depression are associated with different methylation patterns in stress-related biological pathways.
The data do not show that methylation caused depression, and they do not show that changing oxytocin signaling would treat a given patient.
The limitations are central. Injury history was retrospective, and the study did not separately assess brain injury, which could change both psychiatric risk and biology.
Methylation was measured in whole blood, which improves sample size but can miss cell-specific or brain-region-specific patterns. The design also cannot establish whether methylation differences came before injury, followed injury, reflected depression state, or were influenced by medication.
- Best current use: a research lead for trauma-related depression biology.
- Not established: a diagnostic methylation panel for individual patients.
- Next step: longitudinal samples that track injury timing, symptoms, medications, and methylation changes over time.
The oxytocin point is also narrower than it may sound. The study may help explain why oxytocin-based approaches for stress-related disorders have produced heterogeneous results.
If pathway biology differs by diagnosis history and injury exposure, a one-size-fits-all treatment effect would be hard to detect.
Citation: DOI: 10.1016/j.bpsgos.2026.100710. Marshall et al. Methylome-Wide Association Studies of Physical Injury Stratified by Depression Status Assesses Exposure by Diagnosis Effects in Oxytocin Signaling and Synaptic Plasticity. Biological Psychiatry: Global Open Science. 2026.
Study Design: Population-based cohort methylome-wide association and interaction study with pathway-level follow-up analyses.
Sample Size: 4,308 discovery participants and 2,759 participants in an independent pathway-validation sample.
Key Statistic: Traumatic injury was associated with lifetime depression (OR 1.67) and recurrent major depression (OR 2.10), while methylation analyses highlighted oxytocin and synaptic-plasticity pathways.
Caveat: Retrospective injury reporting, whole-blood methylation, and cross-sectional timing mean the findings are biomarker leads, not causal proof or a clinical test.