TL;DR: A 2026 study in Neuropsychopharmacology found that reward uncertainty, measured with functional MRI (fMRI), a brain-scan method, engaged different adolescent brain networks during waiting for a possible reward versus learning the outcome, with anxiety and anhedonia tied to different parts of that response.
Key Findings
- 84 adolescents were scanned: The sample included psychotropic-medication-free youth ages 12-20, including healthy controls and adolescents with mood and anxiety symptoms.
- The task separated certainty from uncertainty: A question-mark cue meant the reward outcome could be 50 cents, 10 cents, or no reward, while other cues told participants the outcome in advance.
- Uncertain cues slowed responses: Reaction time was slower after uncertain cues than certain cues, 697.88 versus 685.73 milliseconds, while accuracy did not significantly differ.
- Anxiety tracked reward-circuit activity: Higher anxiety was linked to lower striatum and thalamus activation during uncertain non-reward expectancy.
- Anhedonia tracked outcome resolution: Greater anhedonia was linked to stronger visual and default-network activity when uncertain outcomes became clear.
Reward uncertainty is not the same thing as reward loss. In this study, adolescents were not gambling against punishment.
They were deciding under a cue that meant the outcome was unknown: a high reward, a low reward, or no reward.
The uncertainty distinction is important for mood and anxiety research. Many everyday choices involve waiting under uncertainty rather than facing a clear win or loss.
A social invitation, a grade, a text reply, or a job callback can all become emotionally loaded before the outcome is known.
Reward Uncertainty Was Tested During Waiting and Outcome Feedback
Researchers used a functional MRI task called the Reward Flanker Task, which measures blood-flow changes while participants respond to letter targets under different reward cues. Functional MRI, or fMRI, is a brain-scan method that uses blood oxygenation as an indirect marker of neural activity.
The study separated two phases:
- Expectancy: The waiting period after a cue, when the adolescent knew either the exact reward value or only that the value was uncertain.
- Attainment: The feedback period after the response, when the adolescent saw what reward was actually earned.
- Valence: The analysis also separated uncertain rewards from uncertain non-rewards, so the analysis was not collapsed into one broad uncertainty score.
The sample included 84 adolescents with a mean age of 15.3 years. Seventeen were healthy controls, 59 had mood and anxiety symptoms, and 8 had externalizing disorders without mood or anxiety symptoms.
Participants were psychotropic-medication-free, which reduces one obvious confound in a reward-processing study. The tradeoff is that the sample was not a routine clinic sample of treated adolescents.
Uncertain Cues Activated Default-Mode Regions and Suppressed Control Regions
During expectancy, uncertain cues produced stronger activity in regions including the posterior cingulate cortex, sensorimotor cortex, superior parietal lobule, lateral occipital complex, and fusiform gyrus.
The pattern crossed several systems:
- Default-mode network: A brain network often involved in internally directed attention, autobiographical thought, and self-referential processing.
- Visual and somatomotor networks: Systems tied to sensory processing and action readiness.
- Frontoparietal control network: A cognitive-control system that showed stronger activation for certain cues than uncertain cues.
In plain terms, the uncertain cue showed a mixed state: more internal monitoring and sensory attention, with less frontoparietal control than certain reward cues.
Behavior fit that interpretation. Adolescents responded more slowly after uncertain cues than certain cues, 697.88 versus 685.73 milliseconds.
Accuracy was similar, 87.26% after uncertain cues and 85.99% after certain cues, so the slower response was not simply a broad performance collapse.
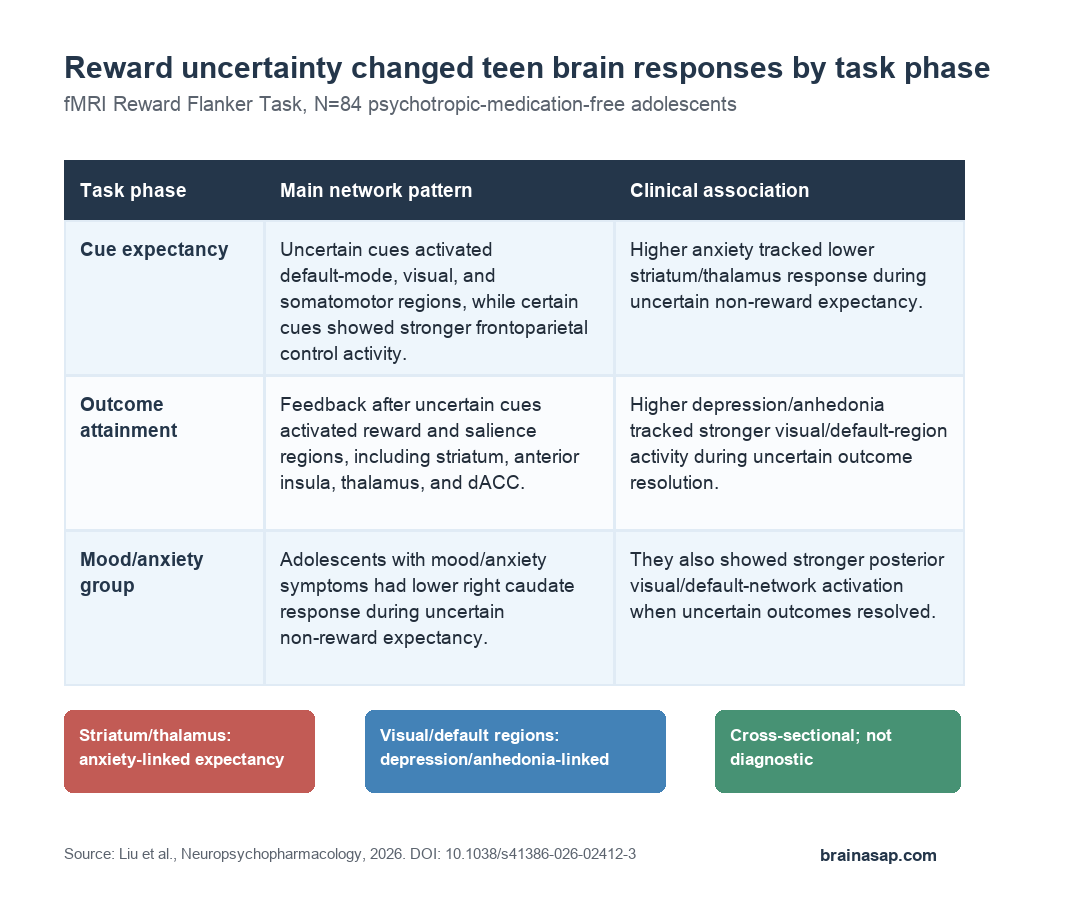
Outcome Feedback After Uncertainty Activated Reward and Salience Regions
The attainment phase looked different. When feedback followed an uncertain cue, stronger activation appeared in reward and salience regions, including the striatum, thalamus, anterior insula, inferior frontal gyrus, lateral occipital complex, cerebellum, and dorsal anterior cingulate cortex.
The strongest broad subcortical cluster included bilateral thalamus, caudate, and putamen. Those structures are relevant because the striatum and thalamus help support reward learning, action selection, and updating behavior after an outcome becomes known.
The researchers also reported that uncertain reward expectancy was intermediate between certain reward and certain non-reward. In other words, the adolescent brain did not treat the question mark as empty.
The question mark cue sat between a known reward and a known no-reward state.
Anxiety and Anhedonia Mapped to Different Uncertainty Signals
The clinical associations were not one generic “more symptoms, more abnormal brain activity” pattern. Different symptoms mapped onto different task phases and regions.
- Anxiety severity: Higher Multidimensional Anxiety Scale for Children scores were associated with lower activation in the bilateral striatum and thalamus during uncertain non-reward expectancy.
- Depression severity: Higher Children’s Depression Rating Scale-Revised scores were associated with stronger lateral occipital activation during uncertain outcome attainment.
- Anhedonia severity: Lower Temporal Experience of Pleasure Scale scores, meaning more severe anhedonia, were associated with stronger lateral occipital and retrosplenial/default-network activation during uncertain outcome attainment.
The anxiety association is especially useful because it points to the waiting period. More anxious adolescents showed a weaker striatal-thalamic response when uncertainty was compared with certain non-reward.
Study authors interpret this as possible evidence that uncertain reward may be appraised less positively in anxiety.
The anhedonia association points to a later moment. When uncertainty was resolved, stronger visual and retrosplenial/default-network activity tracked greater anhedonia.
The retrosplenial cortex is part of the default-mode network, so the finding fits a possible link between outcome resolution and internally directed processing.
The Mood and Anxiety Group Showed Blunted Caudate Response
Exploratory group comparisons separated healthy controls from adolescents with mood and anxiety symptoms. The mood and anxiety subgroup showed lower right caudate activation during uncertain non-reward expectancy.
During uncertain outcome attainment, the same subgroup showed stronger activation in posterior visual regions, including occipital, cuneus, lingual, and fusiform areas.
Those regions are not primary diagnostic markers. They suggest that the group may process the resolution of uncertainty differently.
The group analysis should stay in proportion. The healthy control group had 17 participants, and the mood/anxiety group had 59 participants.
The paper treated those group comparisons as exploratory, not as a ready clinical classifier.
Reward-Uncertainty fMRI Signals Are Not a Clinical Test
This study does not show that an fMRI task can diagnose anxiety, depression, or anhedonia. It also cannot prove that altered uncertainty processing causes later symptoms because the main analysis was cross-sectional.
The stronger takeaway is narrower: uncertain rewards recruited different brain systems during waiting and outcome feedback, and symptom dimensions lined up with different parts of that process.
For adolescent mental health research, the phase split is useful. Anxiety may involve how uncertain reward is appraised before feedback arrives.
Anhedonia may involve how the brain processes the moment when uncertainty resolves. Those are different treatment targets.
Citation: DOI: 10.1038/s41386-026-02412-3. Liu et al. Neural response to reward uncertainty in adolescents with mood and anxiety symptoms. Neuropsychopharmacology. 2026.
Study Design: Cross-sectional fMRI task study using the Reward Flanker Task.
Sample Size: 84 psychotropic-medication-free adolescents ages 12-20, including 17 healthy controls and 59 adolescents with mood and anxiety symptoms.
Key Statistic: Uncertain cues slowed responses compared with certain cues, 697.88 versus 685.73 milliseconds, while accuracy did not significantly differ.
Caveat: The analysis was cross-sectional, group comparisons were exploratory, and the task cannot be treated as a diagnostic test.