TL;DR: A 2026 systematic review and meta-analysis in Acta Neuropsychiatrica found no clear evidence that parenteral clomipramine is better than oral clomipramine for depression or obsessive-compulsive disorder, with low or very low certainty across the main randomized-trial evidence.
Key Findings
- 4,973 publications screened: The review identified 14 randomized controlled trials relevant to parenteral clomipramine in depression or OCD.
- 170 depression patients: Five lower-bias RCTs compared parenteral versus oral clomipramine for depression symptoms within 2 weeks.
- No clear short-term advantage: The pooled 2-week Hamilton Depression Rating Scale difference was -1.27 points, with a 95% CI from -3.09 to 0.54.
- OCD evidence was weaker: Two lower-bias RCTs including 47 patients compared parenteral and oral clomipramine, but heterogeneity prevented meta-analysis.
- Important outcomes were missing: No included RCT reported suicide attempts, mortality, suicidal ideation, global functioning, hospital length of stay, or health-related quality of life.
Source: Acta Neuropsychiatrica (2026) | Ioannou et al.
Parenteral clomipramine means clomipramine given by injection or infusion rather than by mouth. In practice, that usually means intravenous or intramuscular administration.
The rationale sounds plausible: more predictable absorption, faster steady-state levels, and fewer immediate adherence problems. This review asked whether randomized trials actually show better symptom outcomes.
Parenteral Clomipramine Has Been Used Despite Thin Trial Evidence
Clomipramine is a tricyclic antidepressant used for depression and obsessive-compulsive disorder (OCD). The parenteral route has remained in use in some inpatient settings, especially when clinicians want rapid symptom relief or cannot rely on oral dosing.
Researchers framed the question around whether parenteral clomipramine improved depressive or OCD symptoms within 2 weeks, compared with oral clomipramine, other treatments, or placebo.
- Depression group: Eleven RCTs included 317 patients with depression.
- OCD group: Three RCTs included 101 patients with OCD.
- Main measurement: Depression conclusions relied mainly on Hamilton Depression Rating Scale (HDRS) change, while OCD conclusions relied on Yale-Brown Obsessive Compulsive Scale (Y-BOCS) change.
GRADE certainty was central to the review. GRADE is a framework for rating how confident readers should be that an effect estimate is close to the true effect.
Depression Trials Did Not Show Clear Superiority Over Oral Clomipramine
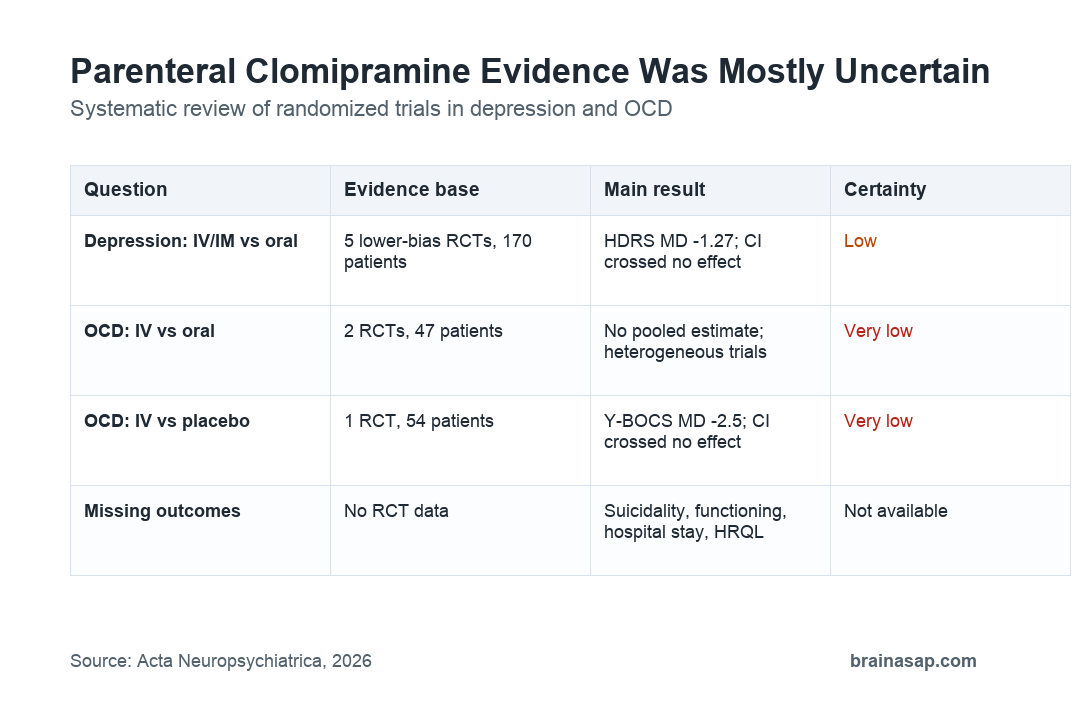
For the main depression question, the evidence came from 5 double-blind RCTs without high risk of bias. Together, they included 170 patients comparing parenteral and oral clomipramine within 2 weeks.
The pooled HDRS change at 2 weeks was -1.27 points favoring parenteral administration, but the 95% confidence interval ranged from -3.09 to 0.54. Because the interval crossed zero, the meta-analysis did not show a clear advantage.
The review also looked at longer-term depression symptoms beyond 2 weeks. The pooled estimate was -1.06 HDRS points, with a wide interval from -4.70 to 2.58 and higher heterogeneity.
OCD Findings Were Too Heterogeneous for a Firm Answer
For OCD, the strongest direct evidence was smaller and more inconsistent. Two lower-bias RCTs with 47 patients compared parenteral with oral clomipramine for OCD symptoms within 2 weeks.
Researchers did not pool those trials because the study designs and patient groups were too different. One placebo-controlled OCD trial in patients poorly responsive to oral clomipramine included 54 patients and reported a Y-BOCS mean difference of -2.5 points, with a 95% confidence interval from -5.6 to 0.6.
- Oral comparator: Existing OCD trials did not establish parenteral superiority over oral clomipramine.
- Placebo comparator: The placebo comparison did not show a statistically clear symptom advantage.
- Evidence certainty: The review rated the OCD evidence as very low certainty because of small samples, inconsistency, and imprecision.
That does not prove parenteral clomipramine never helps an individual patient. It means the randomized evidence is not strong enough to support the route as generally superior.
Missing Outcomes Limit the Inpatient Interpretation
The review’s biggest practical limitation was not just small sample size. Many outcomes that matter in severe inpatient care were absent from the randomized evidence.
- Safety-critical outcomes: No RCT reported suicide attempts, all-cause mortality, or suicidal ideation.
- Function and recovery: No RCT reported global functioning or health-related quality of life.
- Hospital operations: No RCT reported hospital length of stay, even though parenteral use is often discussed in inpatient settings.
Infusion-related adverse events were reported in some trials, including thrombophlebitis and cardiac arrhythmia, but the evidence base was too small and heterogeneous for a clean pooled safety estimate.
Oral Treatment Remains the Default Reading
The review’s practical conclusion was restrained: parenteral clomipramine may not be favorable compared with oral administration, and a short-term depression benefit cannot be fully excluded because the estimates were imprecise.
That is different from saying oral clomipramine is ineffective. The review evaluated the route of administration, not whether clomipramine itself can work for depression or OCD.
Route matters because infusion requires staff time, monitoring, venous access, and management of administration reactions. A treatment route should earn that added burden with evidence that patients do better in ways that matter.
- Best-supported use: Oral clomipramine remains the simpler route when patients can take and absorb medication reliably.
- Possible exception: Parenteral treatment may remain a niche option when oral administration is not feasible or when an inpatient team accepts the uncertainty.
- Research need: New trials would need relevant comparators such as ECT or ketamine and patient-centered outcomes beyond symptom scores.
For now, the evidence does not support routine use of parenteral clomipramine as a superior depression or OCD strategy.
Citation: DOI: 10.1017/neu.2026.10074. Ioannou et al. Parenteral clomipramine for depression or obsessive-compulsive disorder: a systematic review and meta-analysis. Acta Neuropsychiatrica. 2026;38:e30.
Study Design: Systematic review and meta-analysis of randomized controlled trials, with GRADE certainty assessment.
Sample Size: 14 RCTs contributed data; the main depression comparison used 5 lower-bias RCTs with 170 patients.
Key Statistic: Two-week HDRS change for parenteral versus oral clomipramine was -1.27 points, with 95% CI -3.09 to 0.54.
Caveat: Evidence certainty was low or very low, and major outcomes such as suicidality, functioning, hospital stay, and quality of life were not reported.





