TL;DR: A case study published in 2026 in BMC Neurology described a 45-year-old man with acute anti-glycine receptor progressive encephalomyelitis with rigidity and myoclonus (PERM), a stiff-person-spectrum disorder, whose sound-triggered muscle jerks repeatedly drove oxygen saturation down to 30% before immunotherapy and plasma exchange were followed by recovery.
Key Findings
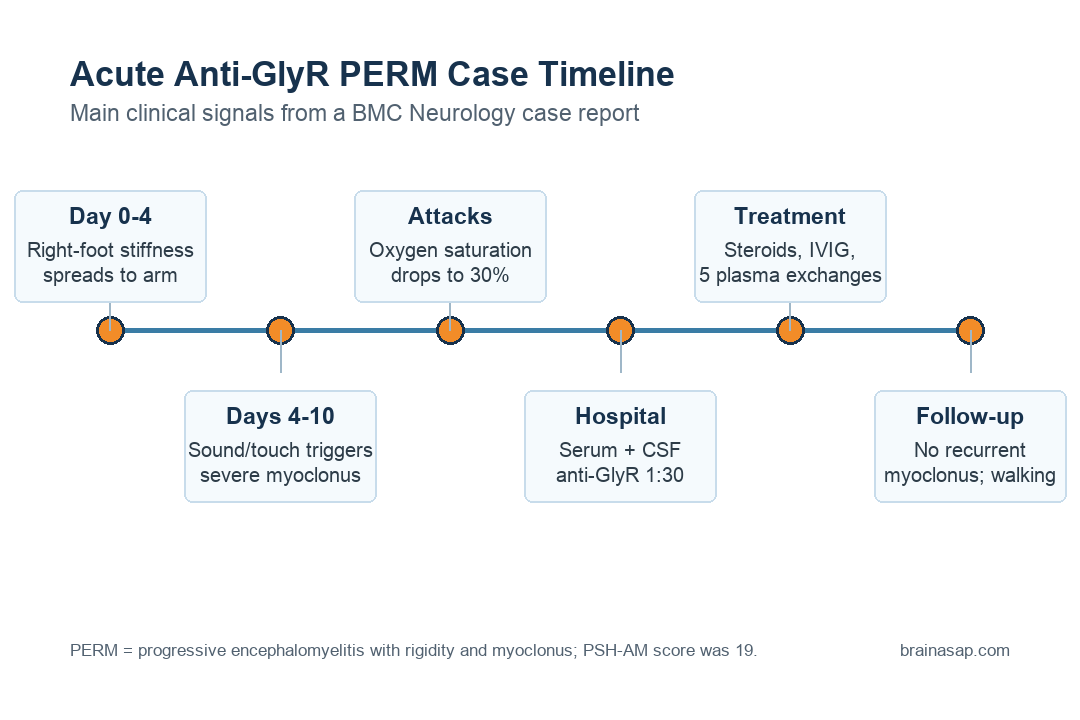
- Acute onset: Symptoms developed over about 10 days, rather than the chronic months-long pattern often described in PERM.
- Respiratory danger: Auditory or tactile triggers set off severe myoclonus, and oxygen saturation dropped to 30% during 3 attacks.
- Immune marker: Anti-glycine receptor (GlyR) antibodies were detected in both serum and cerebrospinal fluid at a 1:30 titer.
- Autonomic storms: Fever, sweating, tachycardia, hypertension, and rigidity produced a PSH-AM score of 19, consistent with likely paroxysmal sympathetic hyperactivity.
- Follow-up: After corticosteroids, IVIG, 5 plasma-exchange sessions, and symptom-control drugs, myoclonus did not recur and the patient could walk independently.
Source: BMC Neurology, 2026.
Progressive encephalomyelitis with rigidity and myoclonus, usually shortened to PERM, sits within the stiff person spectrum. The core pattern is severe stiffness plus myoclonus, which means sudden involuntary muscle jerks.
The important clinical detail in this report was not only that the patient jerked or stiffened. The jerks were stimulus-induced: sound or touch could trigger attacks severe enough to interfere with breathing.
Glycine receptor antibodies matter because glycine is an inhibitory signaling system in the spinal cord, brainstem, and related motor-autonomic circuits. When anti-GlyR autoimmunity is involved, the nervous system may lose part of its normal braking control over muscle activity, brainstem function, and autonomic output.
A Ten-Day Illness Became a Breathing Emergency
The patient was a 45-year-old man who came to the reporting hospital in May 2024 after 10 days of right-limb spasms and pain. The symptoms began in the right foot, where stiffness was accompanied by pes equinus deformity, then spread to the right arm with numbness.
By day 4, fever appeared and the myoclonus worsened. The attacks were mostly triggered by auditory or tactile stimulation, lasted seconds to minutes, and happened multiple times per day.
The breathing risk was direct. During 3 attacks, oxygen saturation fell to 30%, with generalized cyanosis. Clinicians used balloon-assisted ventilation to support the airway and sedatives to control the myoclonus.
Between attacks, the patient showed autonomic instability:
- Heart rate: tachycardia up to 140-160 beats per minute.
- Blood pressure: hypertension up to 140-160/90-100 mmHg.
- Temperature: fever up to 39°C.
- Other signs: excessive sweating, muscle rigidity, and paroxysmal hyperthermia.
Those signs produced a Paroxysmal Sympathetic Hyperactivity Assessment Measure score of 19. Paroxysmal sympathetic hyperactivity (PSH) means episodic overactivation of the sympathetic nervous system, often with fever, sweating, fast heart rate, high blood pressure, and increased muscle tone.
Electroencephalogram Was Quiet, but Anti-GlyR Testing Was Positive
The case could have been mistaken for seizures because the attacks were sudden and dramatic. Video electroencephalogram (EEG), a test that records brain electrical activity, showed no epileptic discharges, and the myoclonus could be triggered by tactile stimulation during monitoring.
The neurological exam showed a wider brainstem and motor syndrome. Researchers reported impaired calculation and memory, ptosis, restricted rightward and downward eye movement, peripheral facial paralysis, dysarthria, right-sided lingual palsy, and muscle strength of 3/5.
The testing pattern separated visible structural imaging from immune evidence:
- Brain MRI: unremarkable.
- Cervical spinal cord MRI: suspicious linear enhancement in the upper cervical segment.
- EMG: co-contraction of agonist and antagonist muscles on admission.
- Antibody testing: anti-GlyR antibodies positive in serum and cerebrospinal fluid at 1:30.
Cerebrospinal fluid cell count was slightly elevated at 19/µL, while CSF protein stayed within the reference range. GAD65 antibodies were negative in CSF, although serum GAD antibodies were mildly elevated.
The reporting team interpreted the low-titer serum GAD finding as possibly nonspecific in the setting of autoimmunity. The stronger diagnostic anchor was the anti-GlyR pattern paired with rigidity, myoclonus, brainstem signs, autonomic dysfunction, and response to immune therapy.
Plasma Exchange Followed Worsening Despite Early Treatment
Before transfer, the patient received antiepileptic therapy, anti-infective agents, sedatives, intravenous methylprednisolone at 500 mg/day for 5 days, and intravenous immunoglobulin at 0.4 g/kg/day. His symptoms continued to worsen by the time he reached the reporting hospital.
Clinicians then used several symptom-control drugs, including clonazepam, baclofen, gabapentin, bromocriptine, and phenobarbital. Methylprednisolone was tapered, and the patient received 5 sessions of plasma exchange.
After the first plasma-exchange session and phenobarbital injection, the frequency of myoclonus decreased and eventually stopped. Anti-GlyR antibodies remained positive at 1:30 after plasma exchange, so the clinical recovery was not simply the same as an immediate antibody disappearance.
Follow-up was encouraging:
- No recurrent myoclonus: Attacks did not return during follow-up.
- Functional recovery: The patient could walk independently and perform activities of daily living.
- Lower antibody titer: At 6 months after discharge, the GlyR antibody titer was 1:10.
Why Breathing Can Fail in Anti-GlyR PERM
Respiratory failure in PERM can come from several mechanisms. The report separates peripheral muscle problems from central brainstem control problems.
Peripheral mechanisms include pharyngeal or respiratory muscle spasms. Central mechanisms involve impaired respiratory rhythm control in the brainstem, where glycinergic signaling helps regulate breathing.
In this patient, the reporting team thought respiratory failure was more likely tied to pharyngeal and respiratory muscle spasm during generalized myoclonus. During attacks, the patient developed inspiratory difficulty, cyanosis, and severe oxygen desaturation, while airway support and myoclonus control improved breathing.
The report also placed the case in a broader PERM literature. One cited cohort found respiratory failure in 18% of anti-GlyR antibody patients, while more recent case reports suggested a higher proportion among selected published cases.
Only some anti-GlyR PERM patients will develop respiratory failure. Trigger-induced myoclonus plus brainstem/autonomic signs should raise the urgency of airway monitoring.
The Case Report Shows a Pattern, Not a Treatment Rule
The strongest practical message is the clinical pattern: acute stiffness, stimulus-triggered myoclonus, brainstem signs, autonomic storms, and anti-GlyR positivity can belong to PERM even when brain MRI and EEG do not explain the attacks.
The treatment conclusion needs more caution. Plasma exchange was temporally linked to improvement, but the patient also received corticosteroids, IVIG, phenobarbital, and other symptom-control medications.
A single case cannot isolate which treatment carried the most benefit.
For clinicians and researchers, the report sharpens a high-risk phenotype. Anti-GlyR PERM can present quickly, can mimic seizure-like events, and can create breathing emergencies when myoclonus recruits airway or respiratory muscles.
The narrow takeaway is clear enough: when PERM is suspected and respiratory compromise appears, early immune testing, airway protection, and prompt immunotherapy may change the outcome.
Citation: DOI: 10.1186/s12883-026-04922-5. Deng et al. Acute onset of progressive encephalomyelitis with rigidity and myoclonus complicated by paroxysmal respiratory failure: a case report. BMC Neurology. 2026.
Study Design: Single-patient neurology case report with literature review.
Sample Size: 1 adult man with acute anti-GlyR PERM and 1-year clinical follow-up.
Key Statistic: Oxygen saturation fell to 30% during 3 stimulus-induced myoclonus attacks; PSH-AM score was 19.
Caveat: The report cannot prove treatment efficacy because immunotherapy, plasma exchange, and symptom-control drugs were used together.





