TL;DR: A 2026 BMC Psychiatry study found that antipsychotic dose was not associated with Montreal Cognitive Assessment (MoCA), a brief cognitive screening test, in clinically stable schizophrenia patients under 40, while higher symptom scores and longer illness duration tracked lower cognition.
Key Findings
- Forty-one clinically stable outpatients with schizophrenia were included after researchers screened a larger community mental-health-center population.
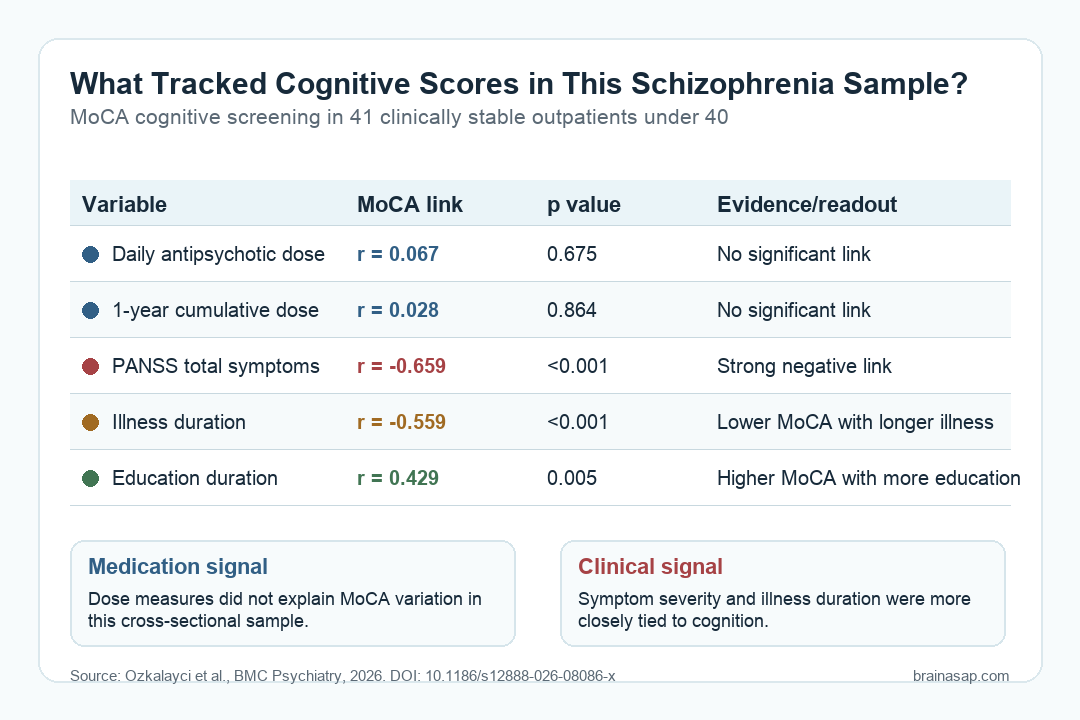
- Daily antipsychotic dose, converted to olanzapine-equivalent milligrams, was not significantly correlated with MoCA cognitive scores (r = 0.067; p = 0.675).
- One-year cumulative antipsychotic exposure also was not significantly correlated with MoCA scores (r = 0.028; p = 0.864).
- PANSS total score, a symptom-severity measure for schizophrenia, had the strongest negative correlation with MoCA scores (r = -0.659; p < 0.001).
- Longer illness duration also predicted lower MoCA performance in the regression model (B = -0.345; p = 0.015).
Dose questions are easy to oversimplify in psychiatric care. A low screening score can reflect current function, schooling, side-effect burden, long-term clinical history, or the treatment plan itself.
This study narrowed the question to a younger and more clinically uniform group. Researchers studied patients ages 20 to 40 with schizophrenia, all followed in one community mental-health center and all clinically stable at routine visits.
The central dose result was negative. In this small sample, higher antipsychotic dose did not explain lower MoCA scores. Symptom severity and illness duration had stronger cognitive links.
Antipsychotic Dose Was Not Linked to MoCA Scores
The medication analysis used two dose measures. Researchers converted each patient’s current daily antipsychotic regimen into olanzapine-equivalent dose, then estimated one-year cumulative exposure using a milligram-by-day calculation from clinical records.
Neither dose measure showed a meaningful relationship with MoCA performance:
- Daily antipsychotic dose: r = 0.067, p = 0.675, Bayes factor 0.260.
- One-year cumulative dose: r = 0.028, p = 0.864, Bayes factor 0.554.
- Number of antipsychotic agents: r = 0.166, p = 0.301.
- Regression model: daily dose was not a significant predictor after accounting for PANSS total score, illness duration, and age (B = 0.023; p = 0.384).
The Bayes factor for daily dose provided moderate evidence favoring no association in this sample. The cumulative-dose result was weaker because the Bayes factor was only anecdotal for the null.
That distinction is clinically useful. The paper does not prove antipsychotics have no cognitive effect in every setting. It says this study did not find a dose-cognition relationship among young, stable outpatients.
Symptom Severity Had the Strongest Cognitive Association
Researchers measured psychotic symptoms with the Positive and Negative Syndrome Scale (PANSS). Higher PANSS scores mean more severe symptoms across positive symptoms, negative symptoms, and general psychopathology.
MoCA scores were lower when symptom scores were higher. The strongest bivariate result was for PANSS total score, which correlated with MoCA at r = -0.659 with p < 0.001.
The symptom pattern was broad:
- PANSS positive symptoms: r = -0.327, p = 0.037 before false-discovery correction.
- PANSS negative symptoms: r = -0.524, p < 0.001.
- PANSS general psychopathology: r = -0.564, p < 0.001.
- PANSS total score: r = -0.659, p < 0.001, with very strong Bayesian evidence.
In the regression model, PANSS total score remained significant after including illness duration, antipsychotic dose, and age. Each higher PANSS total score point was associated with a lower MoCA score estimate.
This is consistent with a clinical reading: cognitive screening results in schizophrenia may reflect current symptom burden, not only medication exposure.
Illness Duration and Education Also Shaped Cognitive Scores
The sample was young, but illness history still varied. The average illness duration was 9.3 years, with a range from 1 to 20 years.
Longer illness duration correlated with lower MoCA scores at r = -0.559. It also remained significant in the regression model, where the estimate was B = -0.345 with p = 0.015.
Two other background variables moved in the expected direction:
- Education duration: longer education was associated with higher MoCA scores (r = 0.429; p = 0.005).
- Age at diagnosis: later diagnosis age was associated with higher MoCA scores (r = 0.473; p = 0.002).
- Mean MoCA score: the sample averaged 20.2 out of 30, below the commonly used cutoff noted by the researchers.
- Clinical stability: participants were stable outpatients, which reduced some acute-episode noise but also limits generalization.
Education and age at diagnosis were not entered into the final regression because they overlapped statistically with age and illness duration.
That does not make them irrelevant. It means the small model could not estimate all of those linked variables cleanly at the same time.
The Sample Was Narrow by Design
Researchers began with 501 clinic patients who had schizophrenia, schizoaffective disorder, or bipolar disorder. After age, diagnosis, education, substance-use, intellectual-disability, neurological, and medical exclusions, 41 patients volunteered and were included.
That selection was intentional. A narrower sample can make the dose question cleaner by reducing clinical heterogeneity.
It also makes the result less generalizable to older patients, first-episode patients, acutely psychotic patients, or people with major neurological and substance-use comorbidity.
The medication context was also specific:
- Second-generation antipsychotics: all patients were taking them, and only one also used haloperidol.
- Combination treatment: 28 of 41 patients used more than one antipsychotic agent.
- Anticholinergic exposure: biperiden use and anticholinergic burden were measured, but neither was significantly associated with MoCA score.
- No benzodiazepines or mood stabilizers: none of the participants were taking these medications, reducing two common cognitive confounders.
The cross-sectional design is the central limit. Because cognition and medication dose were measured at one time point, the study cannot show whether dose changes improve, worsen, or leave cognition unchanged over time.
Clinical Monitoring Still Needs the Whole Picture
The practical takeaway is not that medication dose never has cognitive relevance. It is that therapeutic dosing should not be assumed to be the main reason for cognitive screening differences in every young patient with schizophrenia.
For clinicians and patients, the result points toward broader monitoring. Cognitive complaints may require attention to symptom control, illness course, education and functioning, anticholinergic burden, sleep, depression, substance use, and medication side effects.
A negative dose result can still be useful. It cautions against reducing antipsychotic treatment solely because cognition is low, especially when psychotic symptoms and longer illness duration may be stronger signals.
Larger longitudinal studies are needed to test medication changes over time, use fuller neuropsychological batteries, and compare different antipsychotic profiles.
This study gives a focused cross-sectional answer: in 41 young stable outpatients, antipsychotic dose was not the variable most closely tied to MoCA performance.
Citation: DOI: 10.1186/s12888-026-08086-x. Ozkalayci et al. Antipsychotic dose is not associated with cognitive function in patients with schizophrenia aged under 40: a cross-sectional observational study with retrospective dose estimation. BMC Psychiatry. 2026.
Study Design: Cross-sectional observational study with retrospective one-year medication-dose estimation.
Sample Size: 41 clinically stable schizophrenia outpatients ages 20 to 40.
Key Statistic: Daily antipsychotic dose was not correlated with MoCA score (r = 0.067; p = 0.675), while PANSS total score was strongly negatively correlated with MoCA (r = -0.659; p < 0.001).
Caveat: The sample was small, clinically selected, and cross-sectional, so it cannot prove the cognitive effects of changing antipsychotic dose over time.





