TL;DR: A 2026 retrospective case series study in European Journal of Psychotraumatology found that trauma flashbacks during esketamine nasal spray sessions were distressing but usually time-limited in 22 patients with treatment-resistant depression and PTSD; when treatment continued, depression response was 45.5% and PTSD improvement was 45.5%.
Key Findings
- 22-patient case series: Researchers reviewed adults with treatment-resistant depression (TRD) and comorbid post-traumatic stress disorder (PTSD) who had at least one trauma re-experiencing episode during esketamine sessions across 11 psychiatric departments.
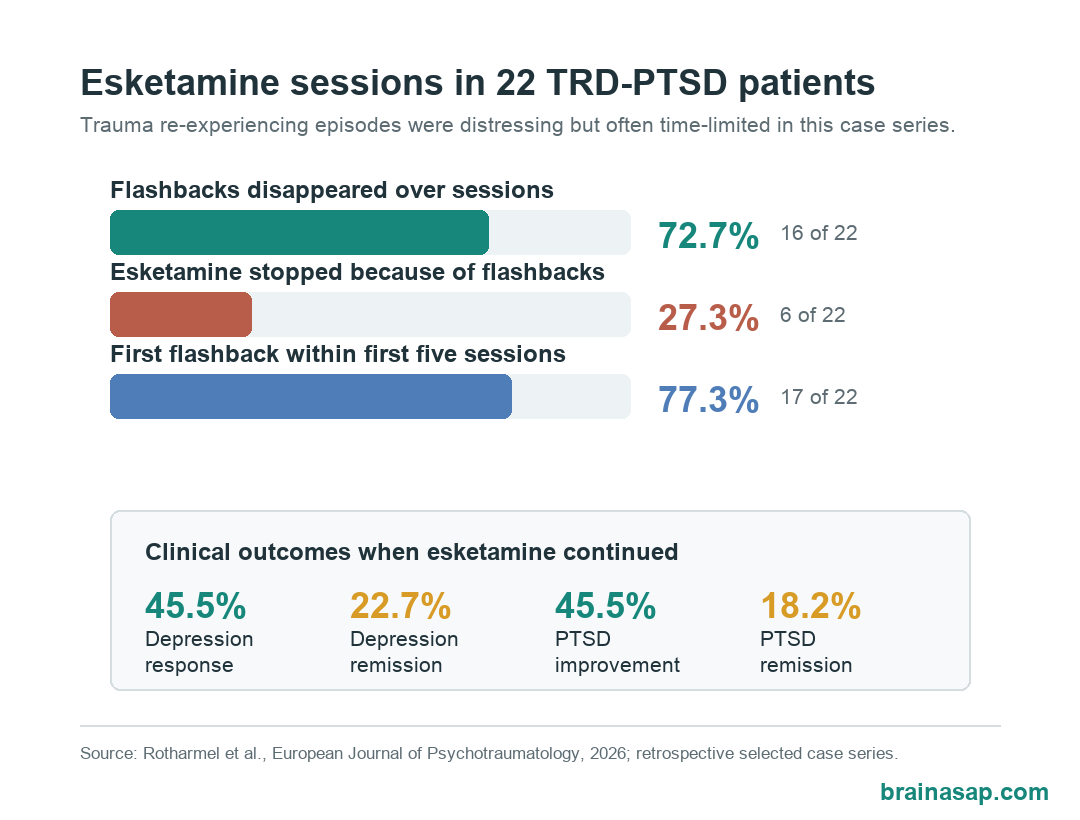
- Flashbacks often appeared early: The first episode occurred at a mean of session 4.4, with 40.9% of patients experiencing it during the first session and 77.3% during the first 5 sessions.
- Most episodes faded with continued treatment: Trauma re-experiencing disappeared as sessions progressed in 16 of 22 patients, or 72.7%.
- Treatment stopped in 6 patients: Esketamine was discontinued because of trauma re-experiencing episodes in 27.3% of the sample.
- Depression and PTSD outcomes improved in some patients: When esketamine continued, depression response was 45.5%, depression remission was 22.7%, PTSD improvement was 45.5%, and PTSD remission was 18.2%.
Source: European Journal of Psychotraumatology (2026) | Rothärmel et al.
Clinically, the question sits between antidepressant treatment and trauma-safety planning.
Esketamine nasal spray is approved for some patients with treatment-resistant depression, but clinicians have much less evidence about patients who also have PTSD.
PTSD can include vivid re-experiencing episodes, often called flashbacks, and esketamine can produce dissociation during monitored treatment sessions.
The Rothärmel team examined what happened when patients with TRD and PTSD had trauma re-experiencing episodes during esketamine care.
Esketamine Sessions Were Reviewed Across 11 Psychiatry Centers
The study was retrospective, meaning researchers looked back through clinical records rather than assigning patients to treatment in advance.
All included patients had moderate-to-severe treatment-resistant depression and comorbid PTSD. Every patient also had at least one clinician-identified trauma re-experiencing episode after esketamine administration that resolved within 2 hours.
The sample was clinically complex:
- Age range: Patients were 21 to 62 years old, with a mean age of 41.8 years.
- Depression type: 16 patients had unipolar depression, while 6 had bipolar I or bipolar II disorder.
- PTSD profile: 19 patients had complex PTSD and 3 had simplex PTSD.
- Suicide history: 17 patients had previous suicide attempts.
- Concurrent therapy: 12 patients were receiving cognitive behavioral therapy (CBT) or eye movement desensitization and reprocessing (EMDR).
Those details limit the conclusions. This was not a routine depression sample; it was a high-severity clinical group already being treated in specialized settings.
Flashbacks Usually Occurred Early and Resolved During Monitoring
Trauma re-experiencing episodes appeared during the peak period after esketamine dosing and resolved before the end of the monitored session.
The first episode occurred early for many patients. 40.9% had a flashback during the first session, and 77.3% had one during the first 5 sessions.
Researchers reported that symptoms were still substantial when these episodes occurred. At the week of flashback onset, mean depression severity on the Montgomery-Asberg Depression Rating Scale (MADRS), a clinician-rated depression scale, was 29.6.
Mean PTSD Checklist for DSM-5 (PCL-5) score, a PTSD symptom questionnaire, was 52.9 among the 9 patients with available scores.
The episodes were not mild for most patients:
- Strong anxiety: 18 patients, or 81.8%, had strong anxiety during the re-experiencing episode.
- Agitation: 7 patients, or 31.8%, showed agitation.
- Crying or release: 12 patients, or 54.5%, reported catharsis with crying and a feeling of release.
- High emotional impact: 21 of 22 patients rated the initial impact as moderate or severe.
The clinical point is not that these events were harmless. They were often intense, and they required supervised care.
Most Trauma Re-Experiencing Episodes Faded With Continued Esketamine
The practical result was the split between patients who continued treatment and those who stopped.
In 16 of 22 patients, trauma re-experiencing episodes disappeared as sessions progressed. In 6 of 22 patients, treatment was stopped because of those episodes.
When esketamine continued, clinical outcomes were mixed but not uniformly poor. Depression response was 45.5%, and depression remission was 22.7%. PTSD improvement was 45.5%, and PTSD remission was 18.2%.
Depression and PTSD outcomes also moved together statistically. Depression response was associated with PTSD response, and depression remission was associated with PTSD remission.
That link does not prove that esketamine treated PTSD directly. A simpler explanation is also possible: when depression improved, PTSD symptoms became easier to manage, or both symptom domains improved in the same patients for overlapping reasons.
Emotional Intensity May Matter for PTSD Improvement
The researchers found one clinically useful pattern in the flashback data.
PTSD improvement was more common when the emotional impact of the flashback was mild or moderate. In that subgroup, the improvement rate was 91.7%.
Among patients whose flashbacks had severe emotional impact, PTSD improvement was 30%.
The pattern fits a cautious exposure-therapy logic, but it should not be overread. The study did not test esketamine-assisted trauma therapy, and the timing of PTSD outcome assessment varied from 1 to 15 months.
Still, the result points to a concrete care issue: clinicians may need to keep the session emotionally tolerable enough for the patient to remain oriented, safe, and supported.
- Too little activation may not engage trauma memory: A mild response may be clinically manageable but may not change symptoms by itself.
- Moderate activation may be workable: The study’s better PTSD outcomes appeared in the mild-to-moderate impact group.
- Severe activation may require stopping or changing care: Severe distress was linked to lower PTSD improvement and drove discontinuation in some cases.
The Case Series Does Not Prove Esketamine Treats PTSD
This paper is useful because it describes a real clinical problem, not because it settles treatment efficacy.
Several limits are important:
- No comparator group: There was no matched group of TRD-PTSD patients without flashbacks or without esketamine.
- Retrospective records: Clinicians identified events from routine care notes, so episode detection was not standardized in advance.
- PTSD measurement varied: PCL-5 scores were available for only 9 patients at flashback onset, and later PTSD improvement relied on clinical judgment.
- Selection bias: The sample only included patients who had trauma re-experiencing during treatment, so it cannot estimate how often flashbacks occur in all TRD-PTSD patients receiving esketamine.
- Small sample: With 22 patients, subgroup patterns can shift substantially if only a few cases change category.
The safest conclusion is narrow. In this case series, trauma flashbacks during esketamine were not automatically a reason that treatment failed, but they were clinically significant events that required monitoring and sometimes stopped treatment.
For future trials, the necessary question is not only whether esketamine improves depression in patients with PTSD. Researchers also need to track trauma re-experiencing prospectively, measure session intensity, and define when continuing treatment is safe.
Citation: DOI: 10.1080/20008066.2025.2609425. Rothärmel et al. Trauma re-experiencing episodes during esketamine treatment in patients with treatment-resistant depression and comorbid PTSD: a retrospective case series. European Journal of Psychotraumatology. 2026;17:2609425.
Study Design: Retrospective multicenter case series from 11 psychiatric departments.
Sample Size: 22 adults with treatment-resistant depression, comorbid PTSD, and at least one trauma re-experiencing episode during esketamine sessions.
Key Statistic: Trauma re-experiencing episodes disappeared over sessions in 16 of 22 patients, while treatment stopped because of the episodes in 6 of 22 patients.
Caveat: No comparator group, small selected sample, retrospective event identification, and variable PTSD outcome measurement limit causal interpretation.