TL;DR: A 2026 meta-analysis in Journal of Medical Internet Research did not find a statistically significant reduction in Patient Health Questionnaire-9 (PHQ-9) depression scores with AI-driven chatbots, but emotionally responsive, structured, and frequent interactions were more consistently associated with user adherence.
Key Findings
- 11 randomized trials: The review included 11 RCTs with 2220 participants for PHQ-9 depression-symptom outcomes.
- Nonsignificant symptom effect: AI chatbot interventions had a pooled SMD of −0.46, with a 95% CI from −1.02 to 0.10.
- High heterogeneity: Clinical-effect heterogeneity was substantial at I²=87%, and the prediction interval ranged from −1.50 to 0.58.
- No overall adherence difference: Pooled adherence did not differ significantly from controls (OR 1.22, 95% CI 0.57 to 2.62).
- Interaction features stood out: High emotional responsiveness, structured feedback, and interaction frequency were associated with higher completion odds in exploratory subgroup analyses.
Source: Journal of Medical Internet Research (2026) | Huang et al.
AI-driven chatbots are increasingly used in depression apps, digital cognitive behavioral therapy tools, and conversational support programs. The 2026 review separated two questions that are often blended together: whether chatbots reduce depressive symptoms, and whether specific interaction designs keep users engaged long enough to complete the intervention.
AI Chatbots Did Not Significantly Reduce PHQ-9 Depression Scores
The meta-analysis included 11 randomized controlled trials of chatbot, conversational-agent, or virtual-therapist interventions for people with depression or depressive symptoms. All included studies measured depressive symptoms with the Patient Health Questionnaire-9 (PHQ-9), a common 9-item depression scale.
The pooled clinical effect favored chatbot interventions, but the confidence interval crossed zero. The standardized mean difference was −0.46, with a 95% CI from −1.02 to 0.10.
Negative SMD values meant larger symptom reduction in chatbot groups. Even so, the conservative Hartung-Knapp-Sidik-Jonkman random-effects analysis did not support a firm overall clinical-effectiveness claim.
- Participants: 2220 people contributed to the depressive-symptom meta-analysis, with 1091 in chatbot groups and 1129 in control groups.
- Outcome scale: PHQ-9 scores were the required depression outcome, which improved comparability across trials.
- Effect estimate: The pooled SMD was in the favorable direction but not statistically significant by the reported confidence interval.
- Certainty rating: The GRADE assessment rated clinical-effectiveness evidence as very low certainty.
Prediction Interval Included No Meaningful Depression Benefit
Heterogeneity was a major part of the result. Clinical-effect heterogeneity reached I²=87%, meaning the included studies varied enough that a single average effect is hard to apply to every future chatbot program.
The 95% prediction interval ran from −1.50 to 0.58. In practical terms, a comparable future trial could find a large favorable effect, a small effect, or no meaningful benefit.
Several sources of variation were plausible:
- Different chatbot systems: Trials used different platforms, including named systems such as Woebot and Wysa as well as other conversational agents.
- Different comparison groups: Control conditions varied across included RCTs, which changes how symptom effects should be read.
- Different user populations: Studies differed in symptom severity, recruitment setting, and intervention context.
- Different interaction designs: Chatbots varied in empathy, feedback, frequency, user choice, and dialogue depth.
The review also assessed small-study effects. For depressive symptoms, funnel-plot asymmetry tests suggested possible bias, and a trim-and-fill adjustment moved the pooled estimate closer to no effect: SMD −0.13, with a 95% CI from −0.47 to 0.21.
Adherence Was Not Higher Overall, but Design Features Differed
User adherence was defined as intervention completion. Across all 11 studies, chatbot interventions did not produce significantly higher adherence than controls: OR 1.22, with a 95% CI from 0.57 to 2.62.
Adherence heterogeneity was also high at I²=74.8%. The prediction interval ranged from 0.24 to 6.18, so completion in future settings could be lower or much higher depending on implementation.
The more useful design analysis came from six coded interaction features:
- Interaction frequency: How intense and regular the user-chatbot exchanges were.
- Emotional responsiveness: How adaptively the chatbot offered empathetic responses.
- Self-disclosure encouragement: How much the chatbot prompted users to share experiences or emotions.
- Dialogue depth: How rich and reflective the conversations were.
- Feedback strategy: Whether the chatbot gave timely, tailored prompts or evaluative responses.
- User agency level: How much control and choice the user had.
Emotional Responsiveness and Feedback Were Linked to Completion
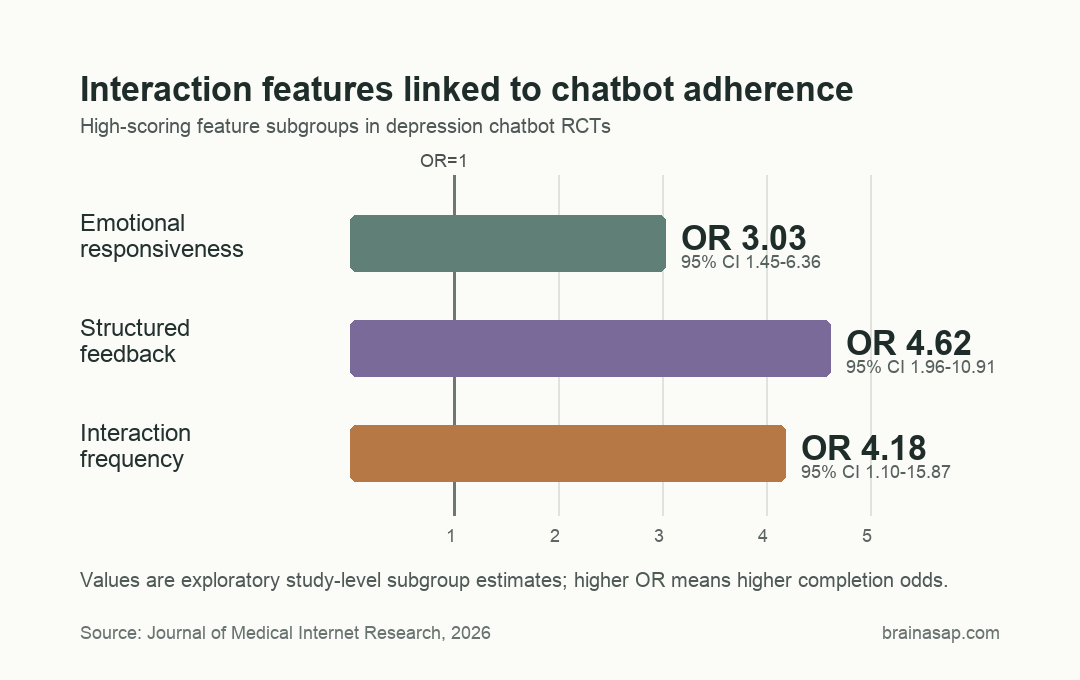
Three features had stronger adherence associations in high-scoring study subgroups. High emotional responsiveness had an adherence OR of 3.03, with a 95% CI from 1.45 to 6.36.
High feedback strategy had an OR of 4.62, with a 95% CI from 1.96 to 10.91.
High interaction frequency also favored completion, with an OR of 4.18 and a 95% CI from 1.10 to 15.87. By contrast, dialogue depth, self-disclosure encouragement, and user agency level had weaker or nonsignificant adherence patterns.
These subgroup findings were exploratory. They were based on study-level coding of published intervention descriptions, not direct measurement of each user’s chatbot conversations.
- Emotional responsiveness: The high-scoring subgroup had stronger completion odds and lower heterogeneity than the low-scoring subgroup.
- Structured feedback: High-scoring studies had the most consistent adherence estimate, with I²=0% in that subgroup.
- Interaction frequency: More regular exchanges were associated with higher completion odds, but the confidence interval was wide.
- Clinical symptoms: Feature associations with PHQ-9 improvement were less stable than feature associations with completion.
AI Therapy Chatbots Need Outcome Proof, Not Just Engagement
The review keeps engagement and clinical benefit separate. A chatbot can be emotionally responsive, structured, and frequently used while still failing to deliver a reliable depression-score improvement across trials.
That distinction is central for digital mental health. Completion may be necessary for benefit, but completion is not the same thing as treatment response.
The limitations are also concrete:
- Small evidence base: Only 11 RCTs were available, limiting subgroup reliability.
- High heterogeneity: Trial results varied substantially for both PHQ-9 change and adherence.
- Study-description coding: Interaction features were coded from published descriptions, not direct logs of chatbot behavior.
- Possible publication bias: Small-study-effect tests weakened the clinical-effect estimate.
Current RCT evidence does not yet show a reliable average PHQ-9 benefit for AI chatbots in depression. The adherence data instead point to interaction design as a possible completion factor.
Future trials need to test design features directly rather than treating the chatbot as a single black-box intervention.
Citation: DOI: 10.2196/88697. Huang et al. Therapeutic Interaction Features of AI Chatbots in Depression Interventions: Systematic Review and Meta-Analysis. Journal of Medical Internet Research. 2026;28:e88697.
Study Design: Systematic review and random-effects meta-analysis of randomized controlled trials.
Sample Size: 11 RCTs with 2220 participants for depressive-symptom outcomes.
Key Statistic: Pooled depression effect SMD −0.46 (95% CI −1.02 to 0.10); pooled adherence OR 1.22 (95% CI 0.57 to 2.62).
Caveat: Evidence certainty was very low for clinical effectiveness because of heterogeneity, imprecision, and possible publication bias.