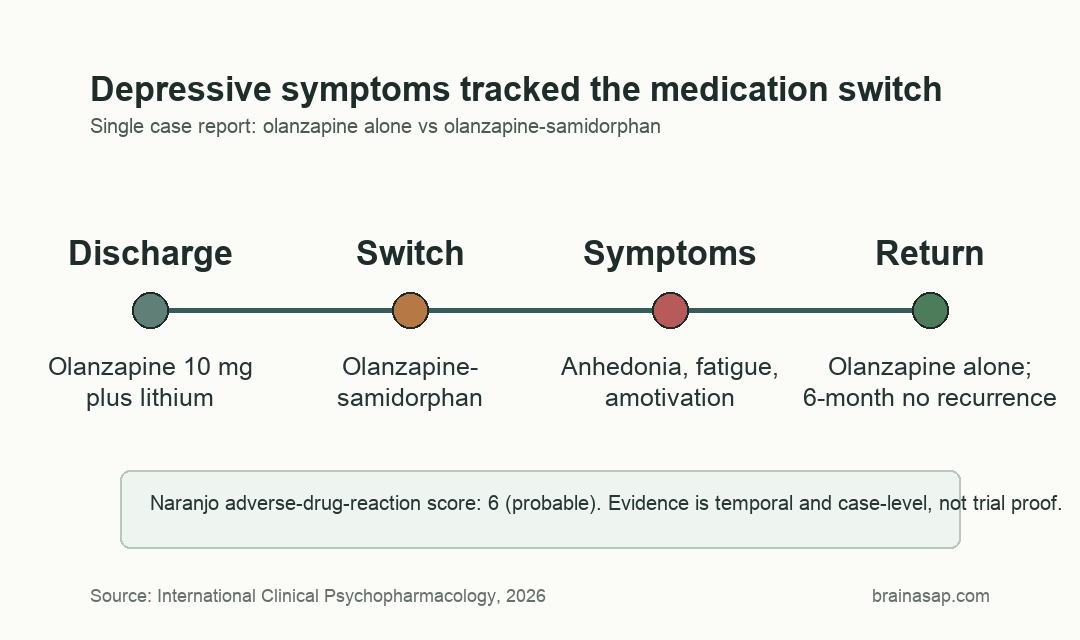
TL;DR: A 2026 study in International Clinical Psychopharmacology described a 40-year-old man whose dysphoria, anhedonia, amotivation, and fatigue appeared soon after olanzapine was changed to olanzapine-samidorphan and resolved after he returned to olanzapine alone.
Key Findings
- One-patient case report: The report followed a 40-year-old man after first psychiatric hospitalization, so the evidence is a clinical signal rather than population-level risk.
- Medication switch: Depressive symptoms emerged after olanzapine 10 mg was changed to olanzapine-samidorphan, a formulation designed to reduce olanzapine-associated weight gain.
- Symptom cluster: The reported mood change included dysphoria, anhedonia, amotivation, fatigue, and a subjective sense of losing emotional range.
- Naranjo score 6: The adverse-drug-reaction assessment scored the event as probable because symptoms followed exposure and improved after discontinuation.
- Six-month follow-up: After resuming olanzapine alone, depressive symptoms resolved rapidly and did not recur over more than 6 months of follow-up.
Source: International Clinical Psychopharmacology (2026) | Parkerson et al.
Olanzapine-samidorphan combines the antipsychotic olanzapine with samidorphan, an opioid-receptor modulator added to blunt olanzapine-associated weight gain. The case report asks a narrower question: whether changing the opioid-signaling part of the formulation could create mood problems in a susceptible patient.
Olanzapine-Samidorphan Was Followed by New Depressive Symptoms
The patient was a 40-year-old man with no previous formal psychiatric diagnosis, no prior manic or depressive episodes, and no family psychiatric history identified in the report. He was hospitalized after several days without sleep, grandiose delusions, disorientation, referential thinking, and functional impairment.
Inpatient clinicians started lithium and olanzapine 10 mg nightly. At a 1-week outpatient follow-up, he and his spouse reported improvement, and symptom ratings were low: a Young Mania Rating Scale score of 2 and a PANSS-6 score of 7.
The medication change came later in outpatient treatment, when olanzapine monotherapy was switched to olanzapine-samidorphan. The stated clinical reason was metabolic risk management, since the patient had a body mass index of 30 at baseline and olanzapine is known for weight-gain liability.
- Initial episode: The hospitalization involved psychosis or possible mania after 3 days without sleep.
- Baseline workup: Head CT, inflammatory markers, thyroid testing, heavy-metal testing, lipid panel, and glucose testing were described as unremarkable.
- Early response: After discharge on olanzapine and lithium, manic and psychotic symptoms were largely controlled at follow-up.
Anhedonia and Fatigue Improved After Returning to Olanzapine Alone
After the medication switch, the patient developed clinically meaningful depressive symptoms. The report names anhedonia, amotivation, dysphoria, fatigue, and loss of emotional range rather than a vague low-mood complaint.
The timeline is the main evidence. Symptoms appeared after exposure to olanzapine-samidorphan, then improved after samidorphan was removed and olanzapine monotherapy was resumed.
Repeat clinical ratings were also low after the return to olanzapine alone: YMRS score 0, PANSS-6 score 6, and MADRS score 5, with no suicidal ideation endorsed. The patient then continued olanzapine alone without recurrence of the mood symptoms for more than 6 months.
- Exposure sequence: Symptoms began after the formulation switch, not during the initial olanzapine response.
- Dechallenge response: Symptoms improved when olanzapine-samidorphan was stopped and olanzapine alone was restarted.
- Adverse-reaction score: The Naranjo scale score was 6, which falls in the probable range.
Opioid-Receptor Pharmacology Is the Proposed Mood Mechanism
Samidorphan was added to olanzapine for a metabolic reason, but it acts in opioid-signaling systems that are also tied to reward, motivation, dysphoria, and mood. The report describes samidorphan as a high-affinity mu-opioid receptor antagonist, with partial kappa-opioid receptor agonist effects and weaker delta-receptor activity.
Mu-opioid receptor blockade alone may not explain the case, because broader naltrexone research has not shown consistent depressive effects in most patients. The kappa-opioid receptor is more relevant to the reported symptom cluster because kappa activation has been linked to dysphoria and anhedonia.
The report also discusses ALKS 5461, a combination involving buprenorphine and samidorphan that was previously studied for depression. Samidorphan’s mood effects may depend on the full receptor mix, the companion drug, dose, and patient vulnerability.
- Mu antagonism: Blocking mu-opioid signaling could theoretically reduce reward tone, but human mood findings for similar antagonists are mixed.
- Kappa activity: Kappa-opioid activation is a plausible route to dysphoria and reduced motivation.
- Combination context: Samidorphan is not acting alone here; it is paired with olanzapine in a patient recovering from an acute psychiatric episode.
- Individual susceptibility: The report supports vigilance for rare mood reactions rather than a claim that all patients face the same risk.
Clinical Monitoring Is the Practical Point for Lybalvi
Olanzapine-samidorphan can still be a useful formulation when weight gain or metabolic risk is a major concern. Large trials have not shown a consistent pro-depressive effect, and this case cannot estimate how often mood symptoms occur.
Monitoring follows directly from the case timeline. Patients starting or switching to Lybalvi may need explicit questions about anhedonia, motivation, fatigue, emotional range, sleep, and suicidal thinking, especially when they have previous depression or other mood-risk factors.
Several limits keep the interpretation narrow:
- Single patient: A case report cannot separate rare drug sensitivity from background clinical fluctuation with the certainty of a controlled trial.
- Recent hospitalization: The patient had just recovered from a first acute psychiatric episode, which complicates attribution.
- Concomitant lithium: Lithium remained part of treatment, so the medication context was not a clean one-drug comparison.
- No rechallenge: The patient was not restarted on olanzapine-samidorphan to see whether symptoms returned, which would have strengthened causal inference but would not necessarily be clinically appropriate.
The most defensible reading is specific: in this case, depressive symptoms followed a switch to olanzapine-samidorphan and improved after samidorphan was removed. That is enough to justify targeted mood monitoring, not enough to conclude that samidorphan commonly causes depression.
Case Reports Can Flag Rare Psychiatric Drug Effects
Rare adverse effects often first appear as carefully described clinical cases. The strength of this report is not sample size; it is the medication chronology, the dechallenge response, and the use of a structured adverse-drug-reaction scale.
For clinicians, the operational step is straightforward. If a patient develops new dysphoria or anhedonia soon after switching from olanzapine to olanzapine-samidorphan, the medication change belongs on the differential diagnosis alongside relapse, sleep disruption, substance use, psychosocial stress, and medical causes.
Citation: DOI: 10.1097/YIC.0000000000000617. Parkerson et al. Samidorphan sadness: does the addition of samidorphan to olanzapine have pro-depressive effects? International Clinical Psychopharmacology. 2026;41:258-263.
Study Design: Single-patient psychiatric case report with medication timeline and adverse-drug-reaction assessment.
Sample Size: 1 adult man recovering after first psychiatric hospitalization.
Key Statistic: Naranjo adverse-drug-reaction score of 6, categorized as probable.
Caveat: The report can flag a plausible adverse reaction but cannot estimate population risk or prove causality.