TL;DR: A 2026 systematic review and meta-analysis in Molecular Psychiatry found that CB-1 receptor blockade and cannabidiol reduced alcohol intake in animal models, but human alcohol-use-disorder evidence remained inconsistent and too thin to support a treatment claim.
Key Findings
- 63 studies reviewed: Researchers synthesized 44 preclinical studies and 19 clinical or human experimental studies of endocannabinoid-system modulators.
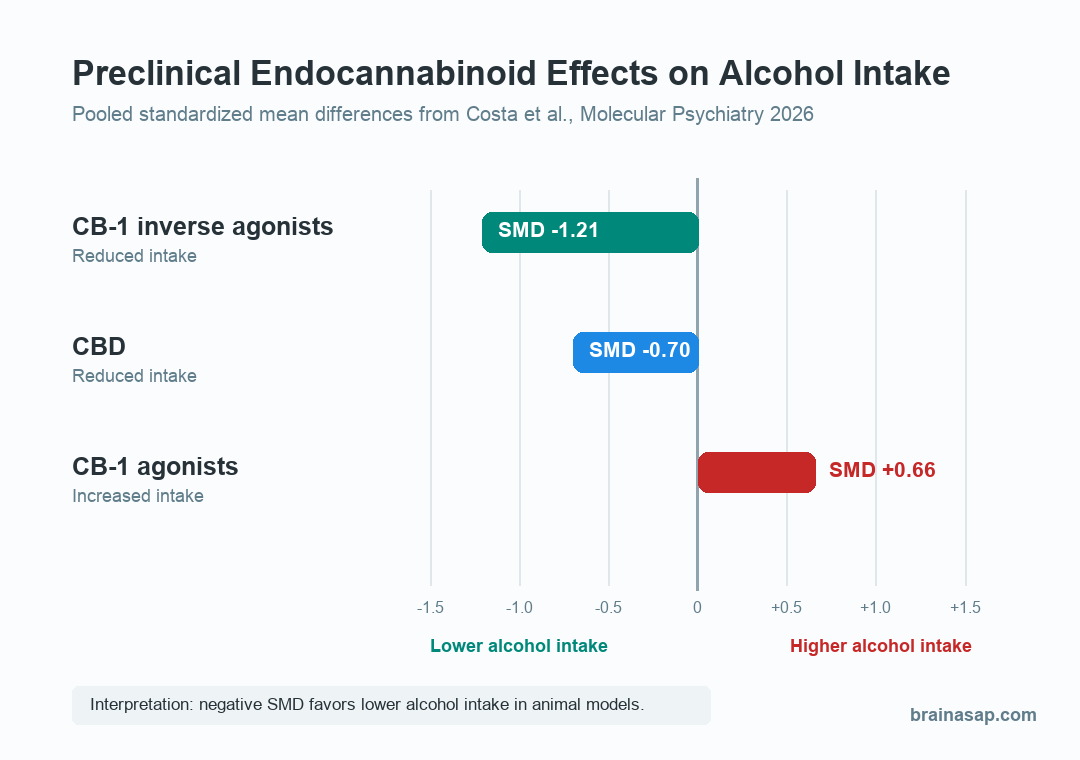
- CB-1 blockade reduced animal drinking: CB-1 receptor antagonists and inverse agonists lowered alcohol intake in preclinical models, with pooled SMD -1.21.
- CBD also lowered intake in animals: Cannabidiol reduced alcohol intake in preclinical models, with pooled SMD -0.70.
- CB-1 agonists moved the wrong way: CB-1 receptor agonists increased alcohol intake in animal studies, with pooled SMD +0.66.
- Human evidence lagged: Clinical studies were heterogeneous, generally null or inconsistent, and mostly focused on rimonabant or CBD rather than newer compounds.
Source: Molecular Psychiatry (2026) | Costa et al.
Alcohol use disorder (AUD) has few approved medication options, and treatment response varies widely. The review tested whether the endocannabinoid system, a signaling system involved in reward, stress, and mood regulation, is a plausible drug target for reducing alcohol use.
The evidence divided by study type. Animal models repeatedly pointed toward some endocannabinoid strategies, especially CB-1 receptor blockade and cannabidiol (CBD). Human studies did not yet show the same clean result.
CB-1 Blockade Reduced Alcohol Intake in Animal Models
The strongest preclinical finding came from drugs that block or suppress CB-1 receptors, one of the main cannabinoid receptor types in the brain. Across 37 experiments in 13 studies, the pooled effect for SR141716A, also known as rimonabant, favored lower alcohol intake.
The meta-analysis reported SMD -1.21, with a 95% confidence interval from -1.59 to -0.83. In practical terms, the animal studies generally found less voluntary drinking or less alcohol self-administration after CB-1 receptor blockade.
- Mechanism tested: CB-1 receptor antagonists or inverse agonists, mostly rimonabant-like compounds.
- Behavior measured: Alcohol drinking, alcohol preference, operant self-administration, or relapse-like alcohol seeking.
- Typical direction: Many studies reported lower intake or weaker alcohol-seeking behavior after CB-1 blockade.
Several studies also found that newer neutral CB-1 antagonists, such as AM4113 and AM6527, reduced alcohol-related behaviors without the same obvious nausea-like, depressive-like, or anxiogenic signals seen with inverse agonist approaches.
This pharmacology distinction is clinically important because the older human CB-1 blocker rimonabant was derailed by psychiatric safety concerns. Blocking a receptor is not identical to pushing its baseline activity below normal, and the review treated that difference as a key future-trial question.
CBD Reduced Animal Drinking, While CB-1 Agonists Increased It
The animal data did not support a simple “more cannabinoid signaling is better” story. CBD and CB-1 agonists moved in opposite directions.
For CBD, the pooled preclinical effect was SMD -0.70, consistent with lower alcohol intake in the included animal experiments. The review also described non-linear dose-response patterns, meaning more drug did not necessarily translate into a simple straight-line benefit.
For CB-1 receptor agonists, the pooled direction was unfavorable: SMD +0.66, indicating higher alcohol intake compared with controls. Some THC-related findings were more complicated, but the overall agonist pattern warned against assuming that cannabinoid receptor activation should reduce alcohol use.
- CB-1 inverse agonists: Lower animal alcohol intake, but older compounds raised psychiatric safety concerns in humans.
- CBD: Lower animal alcohol intake, with possible effects through several receptor and stress-related pathways.
- CB-1 agonists: Higher animal alcohol intake in pooled analysis, making receptor activation a risk signal rather than a straightforward treatment strategy.
Human AUD Studies Did Not Match the Animal Signal
The review could not pool human outcomes in a formal meta-analysis because the studies differed too much. They included laboratory alcohol-administration studies, therapeutic trials, naturalistic observation, different cannabinoid compounds, different doses, and different participant groups.
That human evidence was inconsistent and generally null for alcohol-use outcomes. The authors highlighted that clinical work has mostly tested rimonabant or CBD, while many of the newer or more targeted endocannabinoid compounds remain under-investigated in people with AUD.
- Rimonabant problem: Trials using 20 mg rimonabant did not show clear alcohol-consumption efficacy, and higher exposure is hard to justify because of psychiatric adverse-effect concerns.
- CBD uncertainty: CBD remains plausible, but AUD-specific human studies are still preliminary.
- Clinical bottleneck: The compounds with better preclinical safety logic, including neutral or peripherally restricted CB-1 antagonists, have not been adequately tested in AUD trials.
The review also noted a dosing mismatch. Many animal experiments used acute pretreatment shortly before alcohol exposure, while clinical trials often used daily dosing across weeks.
Acute effects may not predict what happens after repeated exposure, tolerance, or compensatory changes in the endocannabinoid system.
The Treatment Evidence Is Promising but Not Clinically Ready
The practical takeaway is narrow: the endocannabinoid system remains a reasonable AUD treatment target, but the existing evidence is stronger for mechanism selection than for clinical prescribing.
Future trials need to test safer compounds, use alcohol outcomes that match the mechanism, and stratify patients by drinking phenotype, stress reactivity, psychiatric comorbidity, and possibly endocannabinoid biomarkers. Without that design work, another broad AUD trial could miss a subgroup effect or repeat the rimonabant safety problem.
- Better compounds: Neutral CB-1 antagonists, peripherally restricted CB-1 antagonists, FAAH inhibitors, MAGL inhibitors, and CBD-like strategies need clearer human testing.
- Better endpoints: Trials should measure drinking, craving, cue reactivity, stress response, withdrawal symptoms, and relapse-relevant behavior.
- Better monitoring: Psychiatric safety follow-up is essential because mood and stress regulation are part of the same biological system being targeted.
The review does not show that CBD, cannabis, or CB-1 drugs are proven AUD treatments. It shows that one branch of cannabinoid pharmacology repeatedly changed alcohol behavior in animals, while human translation remains the hard, unresolved step.
Citation: DOI: 10.1038/s41380-026-03523-5. Costa et al. Modulating the endocannabinoid system in alcohol use disorder: A translational systematic review and meta-analysis of preclinical and human studies. Molecular Psychiatry. 2026;31:3849-3871.
Study Design: Systematic review and meta-analysis of preclinical alcohol-use models plus narrative synthesis of human studies.
Sample Size: 63 studies total, including 44 preclinical studies and 19 clinical or human experimental studies.
Key Statistic: In preclinical meta-analysis, CB-1 inverse agonists reduced alcohol intake with SMD -1.21, CBD reduced intake with SMD -0.70, and CB-1 agonists increased intake with SMD +0.66.
Caveat: Human AUD evidence remains heterogeneous, limited, and generally inconsistent, so these findings should guide trial design rather than clinical treatment claims.