TL;DR: A 2026 study published in BMC Medicine used lesion network mapping to identify a somatic-symptom brain network centered on the right insula and putamen, then linked atrophy inside that network to somatic symptom severity across 399 psychiatric patients.
Key Findings
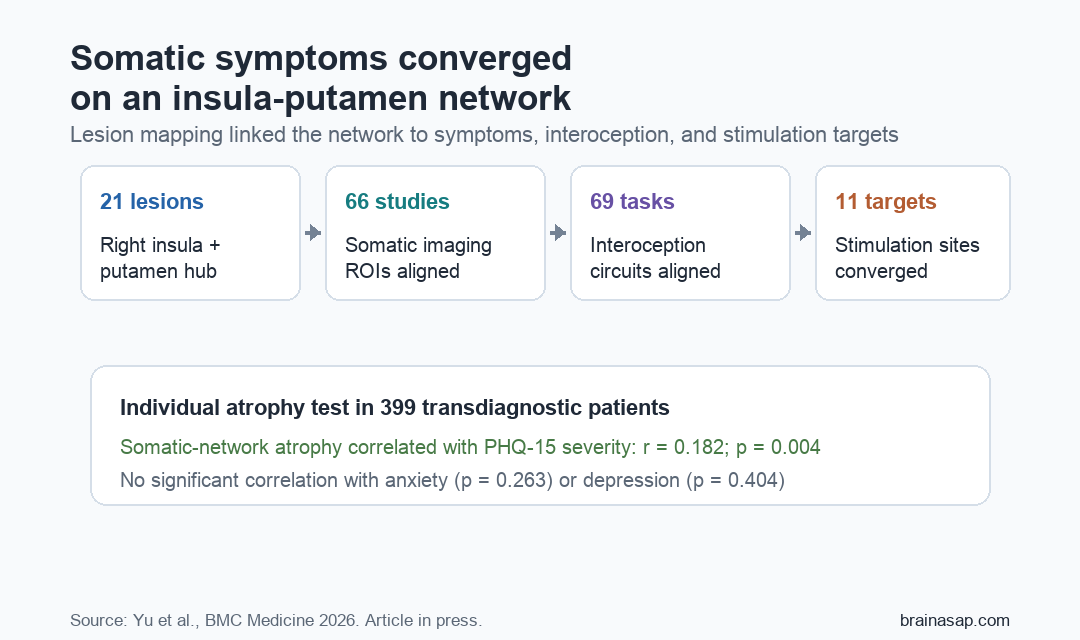
- 21 lesions mapped: Lesions linked to somatic symptoms appeared in different brain locations but converged on a common functional network.
- Right insula-putamen hub: Conjunction analysis identified a hub cluster in the right insula and putamen that was both sensitive and specific to somatic symptoms.
- 66 imaging studies aligned: Independent somatic-symptom imaging regions showed significant connectivity with the lesion-derived network (t=3.297, p=0.002).
- 69 interoception tasks aligned: Interoceptive processing regions showed stronger network connectivity than control regions (F=17.953, p<0.0001).
- 399-patient atrophy test: More atrophy inside the somatic network correlated with PHQ-15 somatic symptom severity (r=0.182, p=0.004), but not anxiety or depression scores.
Source: BMC Medicine (2026) | Yu et al.
Somatic symptoms are distressing bodily complaints that can appear across functional somatic disorders, chronic pain, anxiety, depression, schizophrenia, bipolar disorder, and unexplained medical presentations. This study asked whether those symptoms share a brain-network pattern even when the diagnoses differ.
To test that question, researchers did not rely on one imaging cohort alone. They combined lesion network mapping, independent neuroimaging validation, interoception task data, stimulation-target mapping, and individualized gray-matter atrophy modeling.
21 Somatic-Symptom Lesions Pointed to One Brain Network
Researchers first identified 21 lesion cases from 12 studies in which brain lesions were associated with somatic symptoms. The symptoms included somatoform disorders, chronic pain, palpitations, and excessive somatic preoccupation.
Those lesions were anatomically scattered across cortex, brainstem, limbic regions, subcortical nuclei, and cerebellum. Lesion network mapping then asked whether those different lesion locations were functionally connected to a shared network.
- Discovery connectome: Resting-state functional MRI data from 652 healthy controls in Anhui Province, China.
- Validation connectome: A separate database of 190 patients with somatic symptoms.
- Specificity controls: Networks from 97 non-somatic lesions and randomly generated networks.
- Hub definition: Regions connected to more than 80% of somatic lesions and surviving both specificity tests.
The hub region was located in the right insula and putamen. A broader somatic network built from that hub overlapped most strongly with sensorimotor, subcortical, and ventral attention networks.
Independent Imaging and Interoception Data Supported the Network
The lesion-derived network was tested against independent imaging studies of somatic symptoms. Researchers identified 66 study-level regions of interest from structural and functional imaging papers, covering 2,721 somatic patients and 3,541 healthy controls.
Those somatic imaging regions showed significant functional connectivity with the somatic network (t=3.297, p=0.002). They also connected more strongly to the somatic network than non-somatic control regions or random regions.
Interoception provided a second validation path. Interoception means sensing internal bodily states, and it is central to how bodily symptoms become noticed, interpreted, and regulated.
- 69 task studies: Researchers used regions from a meta-analysis of interoceptive processing tasks.
- Strong network fit: Interoceptive regions connected significantly with the somatic network (t=5.414, p<0.0001).
- Control comparison: Interoceptive regions connected more strongly than non-interoceptive and random regions (both p<0.0001).
Stimulation Targets Converged With the Somatic Network
The study also asked whether known neuromodulation targets for somatic symptoms overlapped with the lesion-derived network. Researchers identified 11 effective stimulation targets from 8 clinical studies using transcranial magnetic stimulation, transcranial direct current stimulation, or transcranial alternating current stimulation.
Those target regions showed significant spatial convergence within the somatic network (t=3.145, p=0.014). A permutation test using 2,000 random networks also found stronger convergence than expected by chance (p<0.0005).
This does not prove that stimulation works through this exact network. It does suggest that previously useful stimulation sites may share a network-level target related to somatic symptom processing.
Somatic-Network Atrophy Tracked PHQ-15 Severity
For individual application, researchers built a normative gray-matter volume model from 1,342 healthy controls. They then applied it to 399 patients with somatic symptoms across anxiety, depression, schizophrenia, and bipolar disorder.
Each patient received a personalized atrophy map, and researchers measured how much atrophy fell inside the somatic network. Greater somatic-network atrophy correlated with Patient Health Questionnaire-15 (PHQ-15) somatic symptom severity (r=0.182, p=0.004).
The association was symptom-specific in this dataset. Somatic-network atrophy did not significantly correlate with Hamilton Anxiety Rating Scale scores (r=0.071, p=0.263) or Hamilton Depression Rating Scale scores (r=0.053, p=0.404).
- Individual maps were heterogeneous: The highest overlap of personalized atrophy locations was only 7%.
- Network filtering helped: Measuring atrophy inside the somatic network extracted a more interpretable symptom-linked component.
- Clinical use remains future-facing: The network has not yet been prospectively used to select treatment targets.
Small Lesion Count and No Prospective Treatment Test Limit the Claim
The strongest claim is mechanistic convergence, not immediate clinical deployment. The lesion sample included only 21 cases, and the source lesions came from published reports with heterogeneous imaging methods.
Lesion network mapping can support causal inference more strongly than cross-sectional imaging, but it still cannot establish absolute certainty without prospective or interventional validation. The stimulation-target analysis also showed spatial overlap, not proof that treatment effects were mediated by this network.
Future studies would need to test whether this somatic network can predict treatment response, guide individualized stimulation targets, or track symptom change over time. For now, it gives researchers a concrete right-insula-putamen-centered network to test across disorders where bodily distress dominates the clinical picture.
Citation: DOI: 10.1186/s12916-026-05044-y. Yu et al. A lesion-derived brain network of somatic symptoms for transdiagnostic individual application. BMC Medicine. 2026.
Study Design: Lesion network mapping study with independent neuroimaging validation, interoception meta-analysis validation, stimulation-target convergence testing, and normative gray-matter atrophy modeling.
Sample Size: 21 lesion cases, 66 independent somatic imaging studies, 69 interoception task-fMRI studies, 1,342 healthy controls, and 399 somatic-symptom patients.
Key Statistic: Somatic-network atrophy correlated with PHQ-15 somatic symptom severity in 399 patients (r=0.182, p=0.004), but not anxiety or depression symptom scores.
Caveat: The lesion set was small, and prospective treatment studies are still needed before the network can be used as a clinical targeting tool.