TL;DR: A 2026 cross-sectional study in Scientific Reports found that attention-deficit/hyperactivity disorder (ADHD) symptom screening was linked to extremely severe chronic pain in 958 adults at Japanese pain centers, while autism spectrum disorder (ASD) screening was not clearly tied to pain intensity.
Key Findings
- Referral pain sample: Researchers analyzed 958 adults with persistent chronic pain despite standard care at multidisciplinary pain centers in Japan.
- ADHD screening rate: 17.1% screened positive on the Adult ADHD Self-Report Scale (ASRS), a self-report ADHD symptom screen.
- ASD screening rate: 4.4% screened positive on the Autism-Spectrum Quotient (AQ), a self-report ASD trait screen.
- Severe pain link: Among people with average pain ratings of 9-10 on a 0-10 numerical rating scale (NRS), 27.4% screened positive for ADHD symptoms.
- Main caveat: The study used self-report screens and cross-sectional data, so it cannot diagnose ADHD or prove that ADHD symptoms caused worse pain.
Source: Kasahara et al. 2026 Scientific Reports study.
ADHD Symptoms Were Common in a Chronic Pain Referral Sample
Chronic pain is not only a body-location problem. For many patients, pain severity is tied to attention, sleep, mood, fear of movement, catastrophizing, and the effort required to keep daily routines going.
The 2026 Scientific Reports study looked at that overlap in a clinical pain population. Researchers studied 958 adults who had persistent chronic pain despite standard care and were making their first visit to multidisciplinary pain centers in Japan.
The sample was not meant to represent every person with chronic pain. These were referral-center patients whose pain had continued despite usual treatment, including medication, nerve blocks, rehabilitation, or other standard care.
Participants completed several self-report measures. The Adult ADHD Self-Report Scale, or ASRS, screened for ADHD symptoms such as inattention and hyperactivity-impulsivity. The Autism-Spectrum Quotient, or AQ, screened for ASD-related traits.
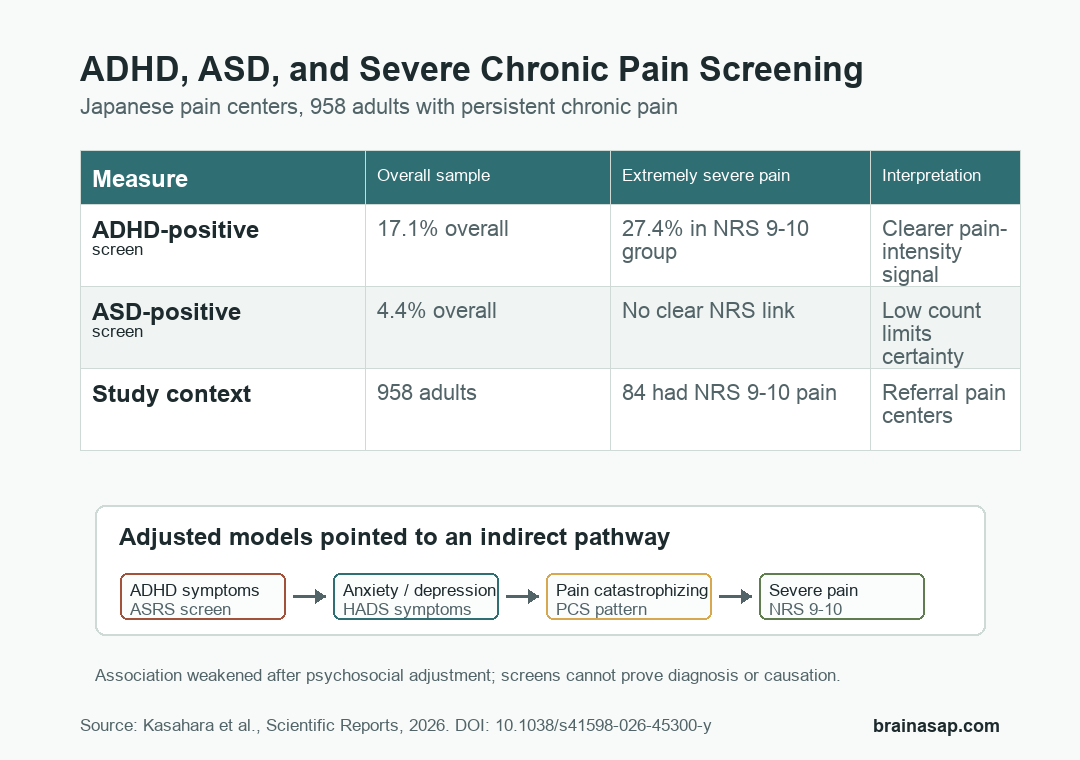
- ADHD symptom screen: 164 of 958 participants, or 17.1%, screened positive on the ASRS.
- ASD trait screen: 42 participants, or 4.4%, screened positive on the AQ.
- Extremely severe pain: 84 participants, or 8.8%, reported average pain of 9-10 on the 0-10 NRS.
Researchers were not saying every chronic pain patient should be labeled with ADHD. The finding was more specific: ADHD symptom screening was more strongly related to pain intensity than ASD screening in this referral-center group.
Extremely Severe Pain Carried More ADHD-Positive Screens
Pain intensity was measured with the numerical rating scale, where 0 means no pain and 10 means the worst pain. Researchers treated average NRS scores of 9-10 as extremely severe pain.
Among all participants, the ADHD-positive screening rate was 17.1%. In the group with extremely severe pain, the rate rose to 27.4%.
The logistic regression results followed the same pattern at first. Before the full psychosocial adjustment, ADHD-positive screening was associated with higher odds of extremely severe pain, while ASD-positive screening was not statistically clear.
That association weakened after researchers added education, anxiety/depression symptoms, insomnia, pain catastrophizing, and pain self-efficacy. In the fully adjusted model, ADHD screening was no longer a significant independent predictor.
The model shift is important. It suggests the ADHD-pain relationship in this sample may run partly through emotional and cognitive pain pathways rather than through ADHD symptoms alone.
Anxiety, Depression, and Catastrophizing Explained Part of the Pattern
The study used several pain-related and mental-health measures to test that idea. The Hospital Anxiety and Depression Scale, or HADS, measured anxiety/depression symptoms.
The Pain Catastrophizing Scale, or PCS, measured repetitive negative pain thinking.
In hierarchical models, adding HADS produced the largest improvement in model fit. Adding PCS also improved the model.
In the fully adjusted model, anxiety/depression and pain catastrophizing remained significant variables for extremely severe pain.
- Initial ADHD signal: ADHD-positive screening was associated with extremely severe pain in simpler models.
- Adjustment changed the result: The ADHD association weakened after anxiety/depression and pain catastrophizing were added.
- Path models supported mediation: ADHD symptoms were linked to severe chronic pain indirectly through anxiety/depression alone, or through anxiety/depression plus catastrophizing.
The path-analysis numbers were modest but clinically coherent. One model estimated an indirect ADHD-to-severe-pain effect of 0.17 through anxiety/depression. Another estimated an indirect effect of 0.13 through anxiety/depression and pain catastrophizing.
The study therefore points toward a practical assessment question. In patients with persistent pain and attention problems, clinicians may need to look at attention symptoms, anxiety/depression, insomnia, catastrophizing, and self-efficacy together instead of treating them as separate issues.
ASD Screening Was More Complicated Than Pain Intensity Alone
ASD screening did not show the same clear relationship with pain intensity. AQ-positive participants had higher levels on several pain-related consequence measures, but average pain intensity and catastrophizing were not clearly higher in the same way.
Researchers cautioned that the AQ may miss some adult ASD presentations, especially in people with pain or few co-occurring psychiatric symptoms. The AQ also has 50 items, which may be burdensome for patients already dealing with pain and fatigue.
- Low ASD-positive count: Only 42 participants screened positive, limiting statistical power.
- Screening limits: AQ positivity is not the same as a clinician-confirmed ASD diagnosis.
- Pain-expression limits: ASD-related pain experiences may show up through function, distress, or behavior rather than higher NRS scores alone.
This is why the ASD result should not be read as “ASD is irrelevant to chronic pain.” A better reading is that the study did not find a clear ASD-pain-intensity signal with this screening approach and sample size.
The Clinical Point Is Screening, Not Causation
The most useful takeaway is straightforward: ADHD symptoms may be worth screening for in patients with persistent chronic pain that has not responded to standard care.
The study does not prove that ADHD caused severe pain. It also does not show that treating ADHD will reduce pain in this population.
Because the design was cross-sectional, symptom direction and timing cannot be established.
Several limits keep the conclusion narrow. ADHD and ASD were assessed with self-report screens rather than structured psychiatric interviews.
Chronic pain itself can affect attention and executive function, which may inflate ADHD-screening scores. The study also lacked detailed information on pain sites and physical functional impairment.
- Screen first: ADHD symptoms may identify patients who need broader psychological and cognitive assessment.
- Treat broadly: Pain care may need anxiety/depression treatment, catastrophizing-focused therapy, rehabilitation, and attention-symptom evaluation.
- Test prospectively: Future studies need clinician-rated ADHD/ASD assessment and longitudinal pain outcomes.
The result fits a biopsychosocial pain model without turning pain into “just psychological” distress. It says that in a difficult referral population, attention symptoms and emotional pain pathways may be part of the same clinical picture.
Citation: DOI: 10.1038/s41598-026-45300-y. Kasahara et al. Attention-deficit/hyperactivity disorder and autism spectrum disorder in chronic pain: a study in Japanese pain centers. Scientific Reports. 2026;16:10544.
Study Design: Cross-sectional screening study at multidisciplinary pain centers in Japan.
Sample Size: 958 adults with persistent chronic pain despite standard care.
Key Statistic: 17.1% screened positive for ADHD symptoms overall, and 27.4% of the extremely severe pain group screened positive.
Caveat: Self-report screening and cross-sectional data cannot confirm ADHD/ASD diagnoses or establish causal direction.





