TL;DR: A 2026 preprint in medRxiv found that a parent-cocreated sensory-reactivity outcome set captured anxiety, mood, sleep, fatigue, cognition, and peer-relationship changes during bumetanide treatment in children and adolescents with neurodevelopmental disorders, but the unmasked design means the results should not be treated as definitive drug efficacy evidence.
Key Findings
- Treatment cohort: 113 children and adolescents ages 7-19 started treatment after enrollment for atypical sensory reactivity plus ASD, ADHD, epilepsy, or tuberous sclerosis complex.
- Seven parent-reported PROMIS domains were tracked: The outcome set measured anxiety, depressive symptoms, sleep disturbance, fatigue, sleep-related impairment, cognitive function, and peer relationships.
- 83% improved on at least one domain: Individual-level analyses found improvement in at least one patient-reported domain for most analyzable participants.
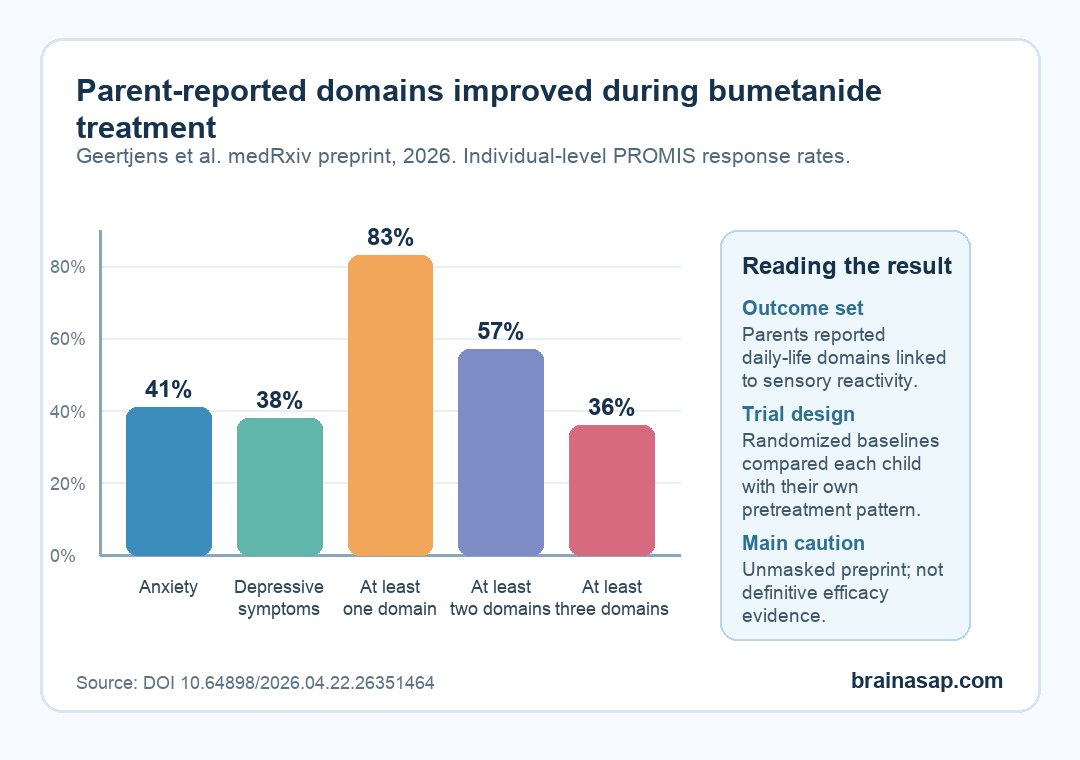
- Anxiety and depressive symptoms changed most often: Improvement appeared in anxiety for 41% of participants and depressive symptoms for 38%.
- Safety events were mostly expected diuretic issues: Orthostatic complaints, hypokalemia, increased urination, headache, dehydration, and dyspepsia were reported, while one sports-related hip fracture was judged probably unrelated.
Source: medRxiv preprint (2026) | Geertjens et al.
Parents Helped Define the Sensory-Reactivity Outcomes
Bumetanide has been studied for autism and related neurodevelopmental conditions because it may influence GABAergic signaling, one part of the brain’s excitation-inhibition balance. Earlier trials produced mixed results, and a broad phase 3 autism trial did not show enough benefit on conventional core-symptom measures.
Researchers tested a different question. Instead of asking whether a standard autism scale could capture every response, they built a parent-cocreated PROMset: a patient-reported outcome measure set chosen to reflect sensory reactivity and daily functioning.
In this study, parents reported on 7 PROMIS domains that could plausibly move with sensory overload or sensory tolerance.
- Mood and anxiety: Anxiety and depressive symptoms were tracked because sensory stress can spill into emotional regulation.
- Sleep and fatigue: Sleep disturbance, sleep-related impairment, and fatigue were included because sensory reactivity can affect daily energy and recovery.
- Cognition and social function: Cognitive function and peer relationships were included because families often notice practical daily-life changes before a diagnostic scale moves.
The study used single-case experimental design (SCED) logic. Each participant had a randomized baseline period of 2-12 weeks, then up to 6 months of bumetanide, with repeated within-person measurements.
The repeated-baseline structure treated each participant’s own pretreatment pattern as part of the comparison, which can be useful in heterogeneous neurodevelopmental populations.
Most Participants Had Large Baseline Daily-Life Impairment
The enrolled group was not a narrow autism-only sample. Participants were 7-19 years old and had atypical sensory reactivity plus a diagnosis of autism spectrum disorder (ASD), ADHD, epilepsy, or tuberous sclerosis complex (TSC).
Of 119 allocated to baseline, 113 started treatment, 102 completed the trial, and 95 had analyzable PROMset data.
Baseline scores showed the outcome set was not measuring a minor side issue. Compared with reference values, participants had substantial impairment across all 7 PROMIS domains.
The largest baseline differences were reported for fatigue, anxiety, and cognitive function.
Sensory reactivity also related to several daily-life domains. Short Sensory Profile scores correlated with anxiety, cognitive function, depressive symptoms, and fatigue at about r = 0.4.
This correlation supports the study’s core premise: sensory reactivity is tied to mood, sleep, energy, cognition, and social participation rather than sitting in a separate symptom box.
Bumetanide Response Was Heterogeneous Across Domains
At the individual level, improvement appeared in 24-41% of participants per PROMIS domain. The most frequent changes were in anxiety and depressive symptoms, with 41% improving on anxiety and 38% improving on depressive symptoms.
Across the whole PROMset, 83% of participants improved on at least one domain, 57% improved on at least two, and 36% improved on at least three.
No participant showed statistically significant worsening on any of the 7 PROM domains.
The largest individual-level response rates appeared in anxiety and depressive symptoms, while the broader PROMset showed that many participants improved in at least one daily-life domain.
The study’s group-level secondary outcomes also moved in the expected direction. Conventional questionnaires improved overall.
Comparisons with historical placebo data favored bumetanide for repetitive behavior and sensory profile scores. Change in sensory profile scores correlated with change in anxiety and depressive symptoms.
- Anxiety response: Anxiety was the most frequently improved PROMIS domain, and large individual effect sizes were common among responders.
- Mood response: Depressive symptoms improved in more than one-third of analyzable participants.
- Multi-domain response: Many children did not improve in only one isolated area, which is why a one-outcome trial could miss part of the response pattern.
The Trial Design Was Sensitive, But Not Definitive
The strongest interpretation is methodological. The study suggests that parent-reported daily-function outcomes plus within-person trial design can detect changes that broad diagnostic scales may miss.
For neurodevelopmental drug development, this is a practical measurement issue because children differ widely in symptom mix, baseline severity, sensory profile, and daily stressors.
The same design also limits causal certainty. The trial was unmasked and did not include a concurrent placebo group.
Some improvement could reflect placebo effects, regression to the mean, spontaneous change, family expectation, pandemic-period context, or nonspecific support during repeated study contact.
Researchers tried to reduce that uncertainty by using randomized baseline lengths, interrupted time-series analyses, randomization tests, historical placebo comparisons, and checks for prior-exposure bias. Those steps make the signal more credible, but they do not replace a blinded placebo-controlled trial.
- Better outcome selection: Future trials may need sensory-linked daily-life domains, not only core diagnostic scales.
- Responder identification: Individual trajectories may help separate children who respond from those who do not.
- Causal testing: A blinded placebo-controlled version would be needed before treating bumetanide as proven effective for these outcomes.
Adverse Events Fit the Diuretic Profile
Bumetanide is a diuretic, so safety monitoring matters. Expected events included orthostatic complaints in 37%, hypokalemia in 36%, increased urination in 35%, headache in 20%, and dehydration in 15%.
These events were generally mild to moderate and resolved.
9 participants discontinued because of adverse events. One had decreasing kidney function, and 8 had diuretic events with mild hypokalemia.
Researchers also reported dyspepsia or decreased appetite in 17% of participants, often resolving after lowering potassium chloride dose.
The practical takeaway is cautious. This preprint does not turn bumetanide into a routine neurodevelopmental treatment.
When sensory reactivity is the clinical target, daily-life domains such as anxiety, sleep, fatigue, cognition, and peer function may be closer to what families actually notice.
Citation: DOI: 10.64898/2026.04.22.26351464. Geertjens et al. Assessing Parent-cocreated Sensory Reactivity Outcomes in Children with Neurodevelopmental Disorders Undergoing Bumetanide Treatment: A Multiple-Baseline Single-Case Experimental Design. medRxiv. 2026.
Study Design: Unmasked multiple-baseline single-case experimental design with randomized baseline periods and 6 months of bumetanide treatment.
Sample Size: 113 participants started treatment; 95 had analyzable PROMset data for the primary outcome.
Key Statistic: 83% improved on at least one PROMIS domain; anxiety improved in 41% and depressive symptoms in 38%.
Caveat: The preprint was not peer reviewed, was unmasked, and lacked a concurrent placebo group, so it cannot prove bumetanide efficacy on its own.