TL;DR: A 2026 paper in Neuropsychopharmacology argued that cannabidiol (CBD), a non-intoxicating cannabis compound, has plausible psychiatric and neurological uses, but clinical claims need standardized products, exposure tracking, and safety monitoring before retail CBD can be treated like medicine.
Key Findings
- Epilepsy evidence is strongest: Approved prescription CBD has the clearest support in rare pediatric seizure disorders, not broad wellness use.
- Psychiatric evidence remains uneven: Early studies suggest possible relevance for anxiety, psychosis, PTSD, and substance use, but many trials are small, short, or product-specific.
- Retail CBD is not one exposure: Products differ by route, formulation, dose, CBD purity, and possible delta-9-THC content, so results from one product cannot be assumed for another.
- Safety depends on context: High-dose or oral CBD can affect liver function, slow metabolism of some medications through CYP450 enzymes, and interact with delta-9-THC.
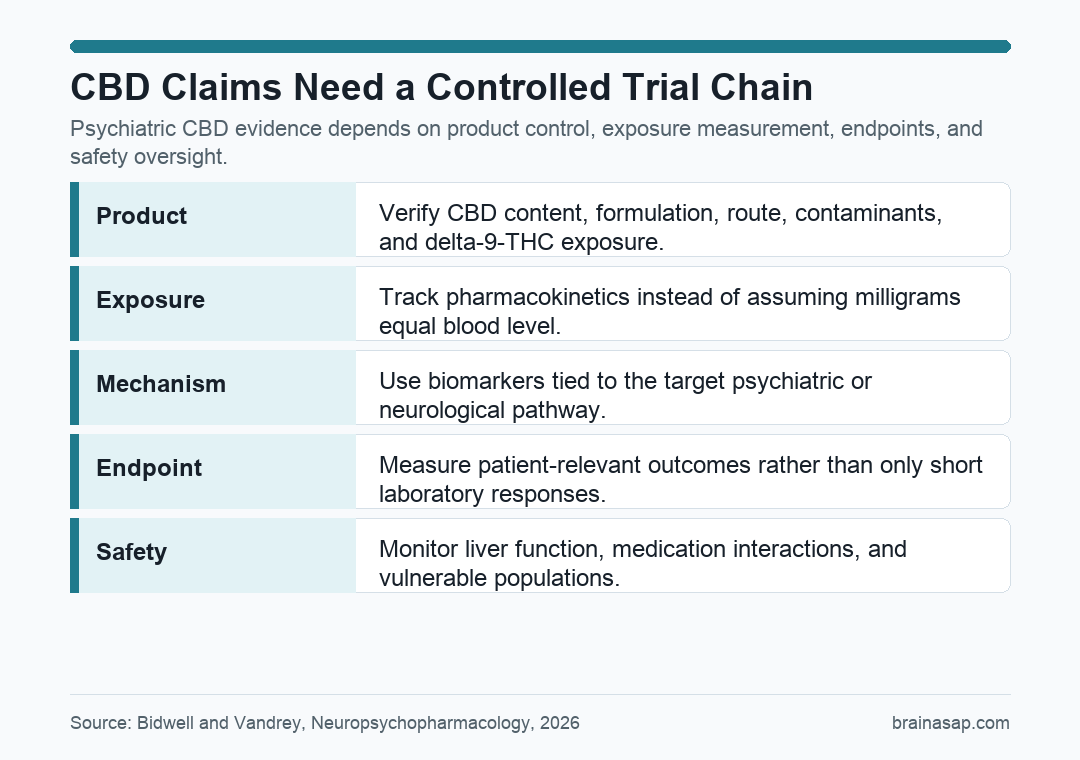
- Translation needs tighter trials: Bidwell and Vandrey called for standardized products, pharmacokinetic monitoring, mechanism biomarkers, clinically meaningful endpoints, and regulatory oversight.
Source: Bidwell and Vandrey, Neuropsychopharmacology, 2026.
CBD is often discussed as if it were one stable treatment. Bidwell and Vandrey’s article says that framing is too loose for clinical decisions.
Cannabidiol (CBD) is non-intoxicating and has low abuse liability, but the paper separates that pharmacology from the much broader market of oils, gummies, inhaled products, topicals, and mixed cannabinoid extracts.
CBD Has Plausible Brain Targets, but Broad Claims Run Ahead of Evidence
Researchers already have reasons to study CBD in brain and mental health disorders. The compound interacts with several systems relevant to mood, stress, reward, pain, and inflammation, including 5-HT1A serotonin signaling, the endocannabinoid system, TRPV1 channels, PPAR signaling, and adenosine pathways.
The clearest clinical success is narrower than the public market suggests. Prescription CBD has regulatory approval for rare seizure disorders such as Lennox-Gastaut syndrome and Dravet syndrome.
Outside that epilepsy context, the evidence is more mixed:
- Opioid use disorder: Prior research has reported reduced cue-induced craving and anxiety after CBD exposure.
- Psychosis research: Some studies have tested CBD as an antipsychotic or adjunctive treatment, with inconsistent evidence across trials.
- Anxiety and PTSD: Early work is biologically plausible, but still depends on product, dose, duration, and outcome choice.
- Youth and vulnerable groups: Lower abuse liability makes CBD worth studying, but tolerability does not prove clinical efficacy.
Biological plausibility is not the same thing as a proven treatment effect. A receptor target can justify a trial; it cannot substitute for one.
Retail CBD Products Make Dose and Exposure Hard to Interpret
The main practical warning is that “CBD” does not describe a single medical exposure. Two products can share the label while giving users very different chemical profiles and blood concentrations.
Product variability appears at several levels:
- Route: CBD can be swallowed, inhaled, applied to skin, or used in other formats, and each route changes absorption.
- Formulation: Oils, powders, capsules, edibles, and botanical extracts can produce different pharmacokinetic profiles.
- Composition: Full-spectrum products may contain delta-9-THC and other cannabinoids, while isolates are closer to CBD alone.
- Regulatory oversight: Retail products may not match clinical-grade products in labeling, quality control, or dose reliability.
Pharmacokinetics means how the body absorbs, distributes, metabolizes, and clears a compound. For CBD, the administered milligram dose often does not cleanly predict systemic exposure, or how much compound reaches the bloodstream over time.
This is why a positive finding for one tested CBD formulation should not be generalized to an unrelated store-bought product.
The clinical question is not just whether CBD was present. It is which CBD product, at what exposure, for which outcome, in which population.
Safety Looks Favorable Only When the Product and Patient Are Known
Bidwell and Vandrey do not frame CBD as a high-abuse drug. Their concern is more specific: safety depends on dose, route, co-use, other medications, and product content.
The paper names three safety issues that clinical CBD research cannot ignore:
- Liver monitoring: Chronic high-dose CBD can affect hepatic function in some patients, especially with age, dose, frequency, and other medications.
- CYP450 interaction: Oral CBD can inhibit drug-metabolizing enzymes, which may slow the clearance of some prescription drugs.
- THC co-exposure: Some retail CBD products contain delta-9-THC, and oral CBD may worsen THC-related adverse effects in certain psychiatric populations.
CYP450 enzymes are liver enzymes that help metabolize many medications. When CBD inhibits those enzymes, another drug’s level may rise, which can increase adverse-event risk.
That is a different message from a blanket “CBD is unsafe” claim. The paper’s position is closer to ordinary pharmacology: a compound can have a useful therapeutic window and still require clinical supervision when doses are high or medication interactions are plausible.
Better CBD Trials Need Product Control and Exposure Data
The integration section gives a clear research roadmap. Future trials need to connect the product a person takes with the biological exposure that follows and the clinical outcome being tested.
The authors’ proposed direction can be reduced to five linked requirements:
- Standardized product: Use well-characterized CBD preparations with verified composition and contaminant control.
- Exposure-informed design: Measure pharmacokinetics instead of assuming dose equals exposure.
- Mechanism biomarkers: Track biological measures that connect CBD action to the target disorder.
- Clinical endpoints: Measure outcomes patients and clinicians actually care about, not only short laboratory responses.
- Regulatory oversight: Separate medical development from loosely labeled retail products.
The practical takeaway is direct. CBD deserves continued study in psychiatry, neurology, pain, and substance-use research, but the evidence is not strong enough to turn most retail CBD claims into medical guidance.
For clinicians and researchers, the disciplined question is not “does CBD work,” but which CBD exposure works for which condition, under which safety controls.
Citation: DOI: 10.1038/s41386-026-02415-0. Bidwell and Vandrey. Cannabidiol at the crossroads: panacea, placebo, or problem? Neuropsychopharmacology. 2026.
Study Design: Circumspective perspective article integrating pro-therapeutic and cautionary views of CBD evidence.
Sample/Model: Not a new participant study; the perspective synthesizes CBD pharmacology, clinical evidence, product variability, and translational trial issues.
Key Statistic: The authors emphasize approved pediatric epilepsy use as the strongest clinical evidence and describe psychiatric uses as promising but insufficiently standardized.
Caveat: This source is an expert perspective, so it guides interpretation and trial design rather than estimating a new treatment effect.