TL;DR: A 2026 crossover study in Clinical Physiology and Functional Imaging found that adding electrical muscle stimulation to low-intensity resistance exercise improved inhibitory control in young men, while stimulation alone showed a delayed 15-minute benefit.
Key Findings
- 17 young men: Participants completed low-intensity resistance exercise, electrical muscle stimulation alone, and combined low-intensity exercise plus stimulation in a randomized crossover design.
- 40% 1-RM exercise: The resistance protocol used bilateral knee extensions at 40% of one-repetition maximum for 4 sets of 10 repetitions.
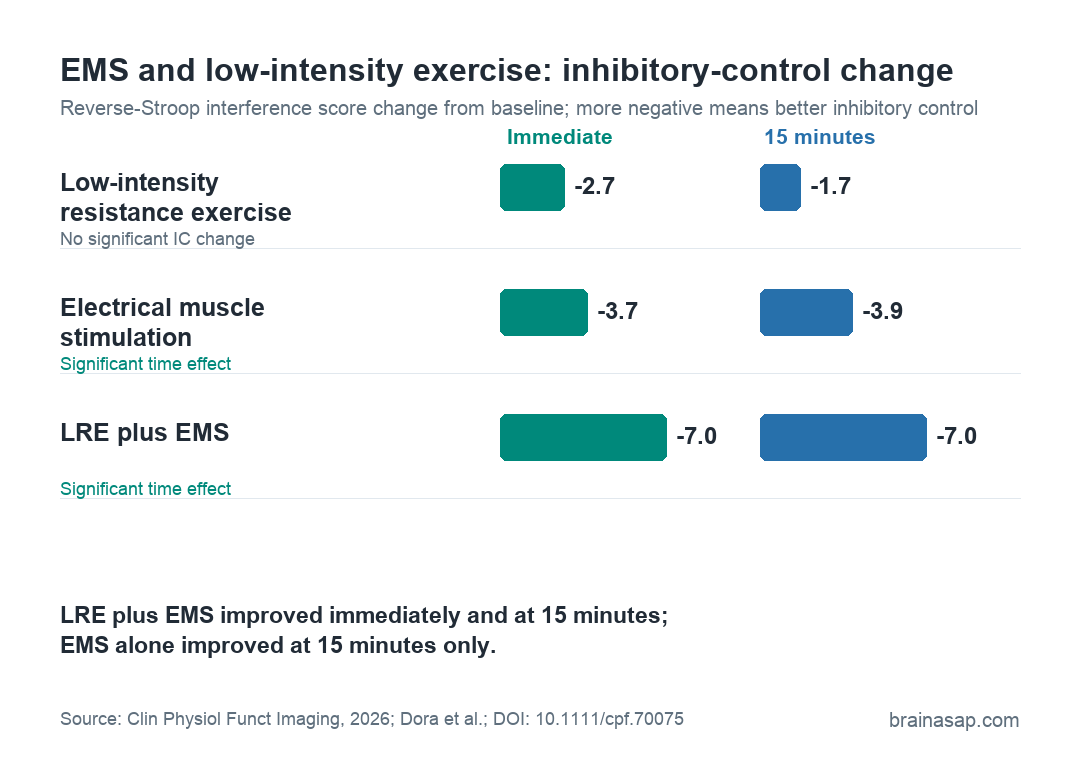
- Inhibitory control improved: LRE plus EMS lowered reverse-Stroop interference scores immediately and 15 minutes after exercise, both with p < 0.001.
- EMS alone had a delayed effect: Electrical muscle stimulation alone did not improve inhibitory control immediately, but did at 15 minutes post-intervention (p = 0.022).
- Effort increased: Combining EMS with low-intensity resistance exercise raised perceived exertion and leg discomfort compared with low-intensity exercise alone.
Source: Clinical Physiology and Functional Imaging (2026) | Dora et al.
Electrical muscle stimulation (EMS) activates motor nerves and lower-limb muscles from outside the body.
This study asked whether electrically driven muscle contraction can shift performance on a cognitive control task.
In healthy young men, the combined protocol improved inhibitory control, the ability to suppress an automatic or inappropriate response.
EMS alone also improved inhibitory control, but only at the 15-minute follow-up test.
Researchers Compared Exercise, EMS, and the Combination
The study used a crossover randomized design, meaning the same 17 participants completed all three experimental conditions on separate days. That design helps reduce between-person noise, because each participant serves as his own comparison.
The 3 conditions were:
- Low-intensity resistance exercise: Bilateral knee extensions at 40% of one-repetition maximum, performed as 4 sets of 10 repetitions.
- EMS alone: Participants sat for 260 seconds while electrical stimulation was applied to the lower-limb muscles.
- LRE plus EMS: Participants performed the same low-intensity knee-extension protocol while receiving electrical muscle stimulation.
Researchers measured blood lactate, blood glucose, perceived exertion, leg discomfort, arousal, mental fatigue, and performance on a color-word Stroop task. The key cognitive outcome was the reverse-Stroop interference score, where lower interference means better inhibitory control.
LRE Plus EMS Improved Inhibitory Control Immediately
The combined condition showed the clearest cognitive result. After LRE plus EMS, reverse-Stroop interference scores were lower immediately after exercise and still lower 15 minutes later. Both comparisons were statistically significant at p < 0.001.
The reported effect sizes were large: d = 1.078 immediately after exercise and d = 1.363 at 15 minutes. The average interference-score change was about -7.0 percentage points at both post-exercise time points.
Low-intensity resistance exercise alone did not show the same pattern. Its time effect for inhibitory control was not significant, with p = 0.100. The mean interference-score changes were smaller, at -2.7 immediately and -1.7 at 15 minutes.
The contrast is the core result. In this protocol, adding stimulation to low-intensity exercise appeared to turn a weak cognitive result into a significant inhibitory-control result.
EMS Alone Showed a Delayed Cognitive Benefit
The stimulation-only condition is the more surprising part of the paper. Participants did not perform voluntary exercise during EMS alone, but inhibitory control still improved by the 15-minute test.
The EMS-alone condition did not significantly differ from baseline immediately after stimulation (p = 0.310). At 15 minutes, however, reverse-Stroop interference was lower than baseline, with p = 0.022 and r = 0.652.
This suggests that electrically induced muscle contraction may have delayed cognitive effects, at least under this short protocol.
The researchers pointed to possible physiological mechanisms, including muscle-derived lactate and stimulation-linked neural activation. The study did not directly prove the brain pathway.
Lactate Rose Most With the Combined Condition
Blood lactate increased in all 3 conditions, but the combined protocol produced the largest rise.
Immediately after the intervention, lactate increased by a median 4.9 mM in the LRE plus EMS condition, compared with 2.1 mM after low-intensity exercise and 1.2 mM after EMS alone.
At 15 minutes, the lactate increase remained larger for LRE plus EMS.
The mean increase was 2.2 mM, compared with 1.0 mM for low-intensity exercise and 0.5 mM for EMS alone.
- Brain-energy hypothesis: Lactate can serve as an energy substrate during neural activation, so a larger lactate response is one plausible contributor.
- Neural-activation hypothesis: EMS may also influence sensory and motor pathways that interact with prefrontal control systems.
- Arousal alone was insufficient: Arousal increased after all conditions, but inhibitory control did not improve after low-intensity exercise alone.
The mechanism remains unresolved. The study measured peripheral lactate and task performance, not real-time prefrontal activity during the Stroop task.
The Added Stimulation Also Raised Effort and Discomfort
The study originally asked whether EMS could make low-intensity exercise more cognitively effective without increasing subjective effort.
That part did not work as hoped. Participants reported greater effort and discomfort in the combined condition.
Mean heart rate was higher during both active exercise conditions than during EMS alone.
Rating of perceived exertion was also higher with LRE plus EMS than with low-intensity exercise alone (p = 0.003), and leg discomfort was higher than in both comparison conditions.
Researchers suggested the stimulation intensity may explain the mismatch. In this study, EMS intensity was set at the maximum level participants could tolerate while maintaining proper knee-extension form.
That may have been high enough to raise lactate, but also high enough to increase local discomfort.
The Result Does Not Yet Generalize to Clinical Populations
The narrow sample is the main boundary. The study included 17 healthy young men, not older adults, women, sedentary adults, stroke survivors, or people with cognitive impairment.
It also lacked a non-exercise control condition, making it harder to completely rule out practice effects on the Stroop task.
Even so, one detail weighs against a pure learning explanation: low-intensity exercise alone did not significantly improve inhibitory control despite repeated task exposure across the experiment.
Short EMS and EMS-assisted resistance exercise may acutely influence inhibitory control, but the protocol needs longer-term testing in more relevant populations.
The next useful test is in people who cannot tolerate higher-intensity voluntary exercise, where EMS might offer more assistance and less relative burden.
Citation: DOI: 10.1111/cpf.70075. Dora et al. The combination of low-intensity resistance exercise and electrical muscle stimulation effectively enhances executive function in men. Clinical Physiology and Functional Imaging. 2026;46:e70075.
Study Design: Randomized crossover acute-intervention study comparing low-intensity resistance exercise, EMS alone, and LRE plus EMS.
Sample Size: 17 healthy young men.
Key Statistic: LRE plus EMS improved reverse-Stroop interference immediately and 15 minutes post-exercise (both p < 0.001); EMS alone improved at 15 minutes (p = 0.022).
Caveat: Healthy young male sample, no non-exercise control condition, and no direct brain-activity measurement during the cognitive task.