TL;DR: A 2026 review in International Journal of Nanomedicine argued that depression nanomedicine should move beyond blood-brain-barrier delivery alone and be judged by target engagement, neuroimmune-barrier-plasticity effects, safety, manufacturability, and patient stratification.
Key Findings
- Mechanism-centered review: The paper organized depression nanomedicine around neuroinflammation, blood-brain-barrier dysfunction, oxidative stress, and impaired neuroplasticity.
- 3 strategy groups: The review grouped current approaches into small-molecule nanodelivery, nucleic-acid nanocarriers, and functional nanoplatforms.
- No routine antidepressant nanoformulation: The authors stated that no nanoformulated antidepressant has entered routine clinical practice for depression.
- Translation bottlenecks: Major barriers included weak patient stratification, limited model relevance, uncertain biodistribution, long-term neurotoxicity, scaling limits, and unclear regulation.
- Precision framework: The proposed path combined barrier-status assessment, liquid biopsy, imaging biomarkers, human-relevant models, and scalable quality control.
Source: International Journal of Nanomedicine (2026) | Wang et al.
Nanomedicine for depression often starts with a delivery problem: how to get therapeutic cargo into or near the brain. This review argues that delivery is only the first screen, not the final proof of therapeutic value.
The authors frame depression as a network disorder involving immune activation, barrier dysfunction, oxidative and mitochondrial stress, glial-neuronal disruption, and impaired synaptic plasticity. In that model, a nanoparticle must do more than cross the blood-brain barrier.
Depression Nanomedicine Was Organized Around a Pathological Network
The review centers on the neuroinflammation-barrier-neuroplasticity axis. That phrase refers to a linked set of processes: inflammatory signaling, blood-brain-barrier changes, neurovascular-unit dysfunction, redox stress, glial changes, and synaptic remodeling.
Rather than sorting the field only by material type—lipids, polymers, exosomes, inorganic particles, or hydrogels—the review evaluates whether each platform is matched to a depression-relevant pathological node.
- Neuroimmune targets: Microglial activation, astrocyte dysfunction, cytokine signaling, and peripheral immune input are treated as therapeutic nodes.
- Barrier targets: The blood-brain barrier is described as an active pathological interface, not just a wall that drugs must cross.
- Plasticity targets: Synaptic remodeling, neurogenesis, trophic signaling, and mitochondrial-redox function are treated as downstream readouts that matter for depression biology.
The core argument is practical: a platform that improves brain accumulation but fails to engage the relevant biological state may not become a credible depression therapy.
3 Nanomedicine Strategy Groups Carried Different Translational Tradeoffs
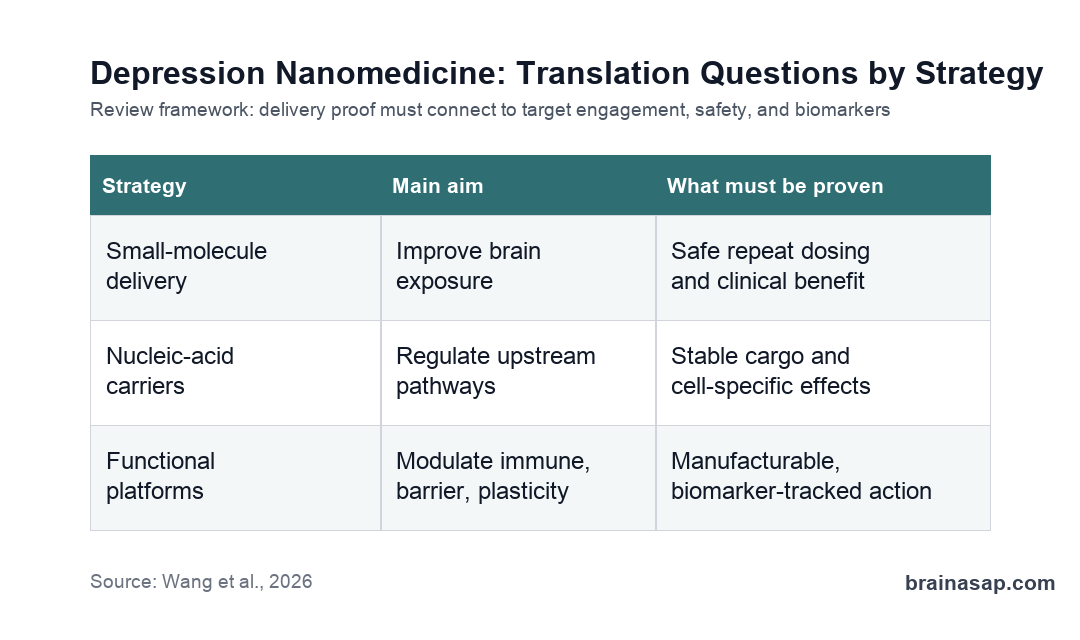
The review divides current strategies into 3 broad groups: small-molecule nanodelivery systems, nucleic-acid nanocarriers, and functional nanoplatforms such as nanozymes, biomimetic membranes, and engineered extracellular vesicles.
Small-molecule redelivery is presented as the most immediately practical route because it can build on known pharmacology and existing drug-safety knowledge. Nucleic-acid and extracellular-vesicle systems may reach narrower molecular targets, but they bring larger manufacturing, stability, immunogenicity, and regulatory challenges.
- Small-molecule nanodelivery: Includes lipid, polymeric, intranasal, and brain-targeted carriers for existing drugs, repurposed compounds, or natural products.
- Nucleic-acid carriers: Includes siRNA, miRNA, and related cargo aimed at upstream inflammatory, barrier, or plasticity regulators.
- Functional nanoplatforms: Includes nanozyme, biomimetic, membrane-coated, and engineered extracellular-vesicle systems designed to combine delivery with biological activity.
The review repeatedly separates preclinical promise from clinical readiness. Many platforms improved depression-like behavior or biological markers in animal and cell models, but that is not the same as durable clinical efficacy in patients.
Blood-Brain-Barrier Delivery Was Not Enough by Itself
The blood-brain barrier is central to the review, but the authors push against a simple delivery-only interpretation. Depression may involve barrier dysfunction, peripheral inflammation, endothelial changes, and neurovascular-unit disruption, so forcing more cargo into the brain is not automatically therapeutic.
For nose-to-brain and barrier-targeted delivery, the review highlights several unresolved engineering problems: nasal mucociliary clearance, human-animal anatomical differences, dose scalability, mucosal safety, formulation reproducibility, and quantitative biodistribution.
- Barrier status: Patients may differ in whether barrier repair, barrier bypass, or controlled local delivery is the more rational approach.
- Biodistribution: Brain entry must be measured regionally and repeatedly, not inferred from a single animal endpoint.
- Safety: Long-term mucosal, immune, vascular, and neurotoxicity data are needed for repeated administration.
This narrows the field’s evidence standard. A carrier that crosses a barrier in a rodent model still has to show safe, reproducible, disease-relevant activity in a human treatment pathway.
No Nanoformulated Antidepressant Is Routine Clinical Care
The strongest clinical boundary in the review is direct: no nanoformulated antidepressant has become part of routine clinical practice for depression. Most evidence remains in material design, cellular validation, animal models, or proof-of-concept translational studies.
The paper lists several barriers that would have to be solved before depression nanomedicine could become a credible precision-therapy route.
- Patient stratification: Depression subtypes need biomarker definitions, such as inflammatory, barrier-damage, or plasticity-deficient profiles.
- Model relevance: Rodent stress and inflammation models do not fully capture human depression heterogeneity.
- Manufacturing: Batch-to-batch variability, cargo instability, scaling, and quality control can make complex platforms hard to translate.
- Regulation: Combination products, biologic cargo, engineered vesicles, and multifunctional platforms may not fit simple drug categories.
Those limits make the review more grounded than a promotional overview. It describes where the science is moving while keeping the clinical bar visible.
Precision Depression Nanomedicine Needs Biomarker-Guided Testing
The proposed framework is biomarker-guided and patient-specific. Future studies would assess blood-brain-barrier status, liquid-biopsy markers, imaging readouts, target engagement, and network-level biological effects before claiming a platform is disease modifying.
The authors also emphasize human-relevant validation models, including blood-brain-barrier chips, patient-derived cerebrovascular-unit models, and glia-neuron co-culture systems. These models could reduce the gap between animal proof-of-concept and human treatment studies.
The clinical message is conservative. Depression nanomedicine may eventually become a precision tool, especially for biologically defined subtypes, but the field still needs reproducible efficacy, long-term safety, scalable manufacturing, and interpretable biomarkers before moving from advanced concept to treatment option.
Citation: DOI: 10.2147/IJN.S617617. Wang et al. Nanomedicine for Depression: From Blood-Brain Barrier Delivery to Neuroimmune-Barrier-Plasticity Network Reprogramming. International Journal of Nanomedicine. 2026;21:617617.
Study Design: Mechanism-oriented integrative review of depression nanomedicine platforms, pathophysiology, preclinical evidence, and translational barriers.
Sample/Model: Review of peer-reviewed studies involving depression pathophysiology, nanodelivery systems, animal and cell models, biomarker concepts, and translational frameworks.
Key Statistic: The review groups strategies into 3 major classes and states that no nanoformulated antidepressant is currently part of routine clinical practice for depression.
Caveat: The paper is a narrative/integrative review, not a clinical trial or meta-analysis, so it synthesizes direction and barriers rather than estimating treatment efficacy.