TL;DR: A 2026 Critical Care Explorations paper described a 17-year-old girl whose intentional lisdexamfetamine overdose was followed by delayed severe heart failure, with left ventricular ejection fraction falling below 20% before recovery over months.
Key Findings
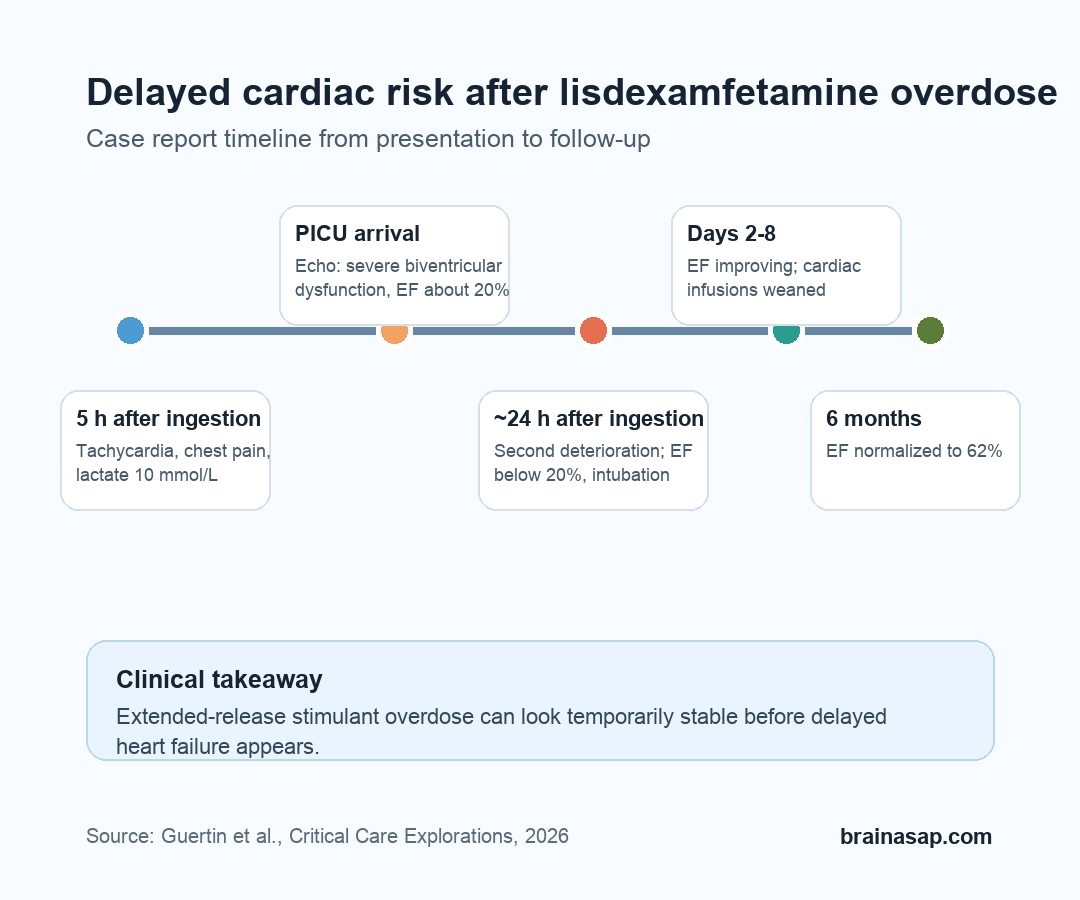
- Delayed cardiac collapse: The patient first appeared stable after treatment, then worsened again about 24 hours after ingestion.
- Severe but reversible dysfunction: Echocardiography showed left ventricular ejection fraction below 20%, later normalizing to 62% at 6 months.
- Extended-release risk: Researchers argued that delayed absorption from a very large stimulant ingestion may have contributed to the second wave of toxicity.
- Monitoring implication: Rising troponin, lactic acidosis, hypoxia, or hemodynamic instability after extended-release amphetamine overdose should prompt early cardiac evaluation.
- Evidence boundary: The report is clinically useful, but it remains one case without measured lisdexamfetamine blood levels.
Source: Critical Care Explorations, 2026.
Lisdexamfetamine is a prodrug stimulant used to treat attention-deficit hyperactivity disorder (ADHD), meaning the body converts it into active dextroamphetamine after ingestion. In routine use, that conversion helps create a smoother medication course than immediate-release stimulants.
In overdose, the same extended-release profile can become clinically awkward. The drug may keep feeding a sympathomimetic toxidrome, a high-adrenaline toxicity pattern marked by agitation, dilated pupils, high blood pressure, rapid heart rate, movement symptoms, and sometimes seizures.
A 1,000 mg Lisdexamfetamine Ingestion Led to a Biphasic Course
The case involved a 17-year-old girl who arrived at a pediatric emergency department about 5 hours after intentionally ingesting about 1,000 mg of lisdexamfetamine, described as fifty 20 mg capsules. She had chest pain and nausea, with tachycardia in the 110-130 beats/min range and mild hypertension.
Researchers reported psychiatric and medical context, including major depressive disorder, post-traumatic stress disorder, generalized anxiety disorder, ADHD, and asthma. Her other prescribed medications were accounted for, and toxicology screening for several common co-ingestants was negative.
- Initial vital signs: Tachycardia and mild hypertension were present, but she was normothermic and initially alert.
- Early bloodwork: Lactate reached 10 mmol/L, with acidosis and elevated high-sensitivity cardiac troponin I.
- Early treatment: Clinicians started supportive care with IV fluids, benzodiazepines, and nausea treatment.
The first major warning sign was not just agitation or hypertension. She developed hypoxia, pulmonary rales, diffuse chest x-ray infiltrates, rising troponin, and point-of-care ultrasound evidence of reduced left ventricular function.
Heart Function Fell Below 20% Before It Recovered
In the pediatric intensive care unit, echocardiography showed severely decreased biventricular systolic function, with left ventricular ejection fraction around 20%. Ejection fraction is the percentage of blood the left ventricle pumps out with each beat; a value near 20% represents severe systolic dysfunction.
The team treated the patient as acute heart failure with stimulant toxicity and possible coronary vasospasm. Management included nitroglycerin, milrinone, benzodiazepines, respiratory support, and close monitoring.
The course then became more concerning because she worsened after an apparent period of stability. On post-admission day 1, after roughly 16 hours of relative stability, she developed recurrent hypertension, severe tachycardia above 170 beats/min, hypoxia, a brief loss of consciousness, and another troponin rise.
- Cardiac imaging: Repeat echocardiography showed left ventricular ejection fraction below 20%, septal dyskinesis, and a dilated left ventricle.
- Respiratory support: Persistent instability led to intubation, with the extracorporeal membrane oxygenation team on standby.
- Organ stress: Bloodwork showed kidney, liver, muscle, and potassium abnormalities during the worst phase.
Recovery was gradual. Ejection fraction improved to the mid-20s by post-admission day 2, reached about 30% by extubation on day 4, and later normalized to 62% at 6-month follow-up.
Why an Extended-Release Stimulant Can Worsen Late
The key clinical point is timing. The reported deterioration did not fit a simple one-peak stimulant overdose.
Researchers emphasized that extended-release or prodrug stimulant ingestions may produce delayed or prolonged toxicity, especially when the dose is very large.
One proposed mechanism was delayed absorption. A large quantity of capsules may contribute to pharmacobezoar formation, meaning a clumped mass of medication material in the gastrointestinal tract that can keep releasing drug.
Researchers also suggested that poor bowel perfusion during heart failure could alter absorption, then improved circulation during treatment might allow another wave of drug uptake.
- Large dose: About 1,000 mg of lisdexamfetamine created a much larger exposure than normal therapeutic use.
- Delayed absorption: Extended-release behavior and possible medication clumping could keep active drug entering the body.
- Changing perfusion: Acute heart failure can reduce gut blood flow, while treatment can restore perfusion and potentially change absorption again.
This does not prove a pharmacobezoar occurred in this patient. It gives clinicians a practical explanation for why stimulant toxicity can look better and then worsen again when the exposure is large and prolonged.
Cardiac Monitoring Should Not Wait for Shock
The case report argues for early cardiac attention when extended-release amphetamine overdose has red flags. A normal initial impression should not end monitoring if the patient has chest pain, rising troponin, lactic acidosis, hypoxia, abnormal blood pressure, or signs of poor perfusion.
Researchers recommended evaluation that can include electrolytes, troponin, end-organ function testing, electrocardiogram, and early echocardiography when the clinical picture suggests cardiac involvement. The point is not to echocardiogram every mild stimulant exposure; it is to avoid missing acute heart failure in the subset with objective warning signs.
- Troponin rise: A cardiac injury marker can help separate routine tachycardia from myocardial stress.
- Lactic acidosis: High lactate may reflect severe physiologic stress, poor perfusion, or both.
- Hypoxia or pulmonary edema: Respiratory decline can be a heart-failure clue, not only aspiration or infection.
- Delayed recurrence: Extended-release stimulant overdose may require continued observation even after early improvement.
The limitations are important. This is a single case report, lisdexamfetamine levels were unavailable, and unreported co-ingestion cannot be completely excluded.
Viral testing was positive for enterovirus/rhinovirus, although the rapid cardiac recovery made myocarditis less likely in the treating team’s interpretation.
Still, the case gives a clear bedside warning: severe stimulant overdose can become a heart-failure problem, and the highest-risk period may extend beyond the first few hours.
Citation: DOI: 10.1097/CCE.0000000000001401. Guertin et al. Sympathomimetic Overdose With Lisdexamfetamine in a Pediatric Patient Resulting in Stress Cardiomyopathy-A Case Report. Critical Care Explorations. 2026.
Study Design: Pediatric case report of intentional extended-release stimulant ingestion.
Sample Size: 1 patient, a 17-year-old girl.
Key Statistic: Left ventricular ejection fraction fell below 20% during deterioration and normalized to 62% at 6-month follow-up.
Caveat: The report cannot prove causality or rule out every possible contributor because drug levels were unavailable and co-ingestion cannot be completely excluded.