TL;DR: A 2026 network meta-analysis in International Clinical Psychopharmacology found that lurasidone and xanomeline-trospium improved global cognitive scores in schizophrenia-spectrum randomized trials, while quetiapine and cariprazine ranked best for attention.
Key Findings
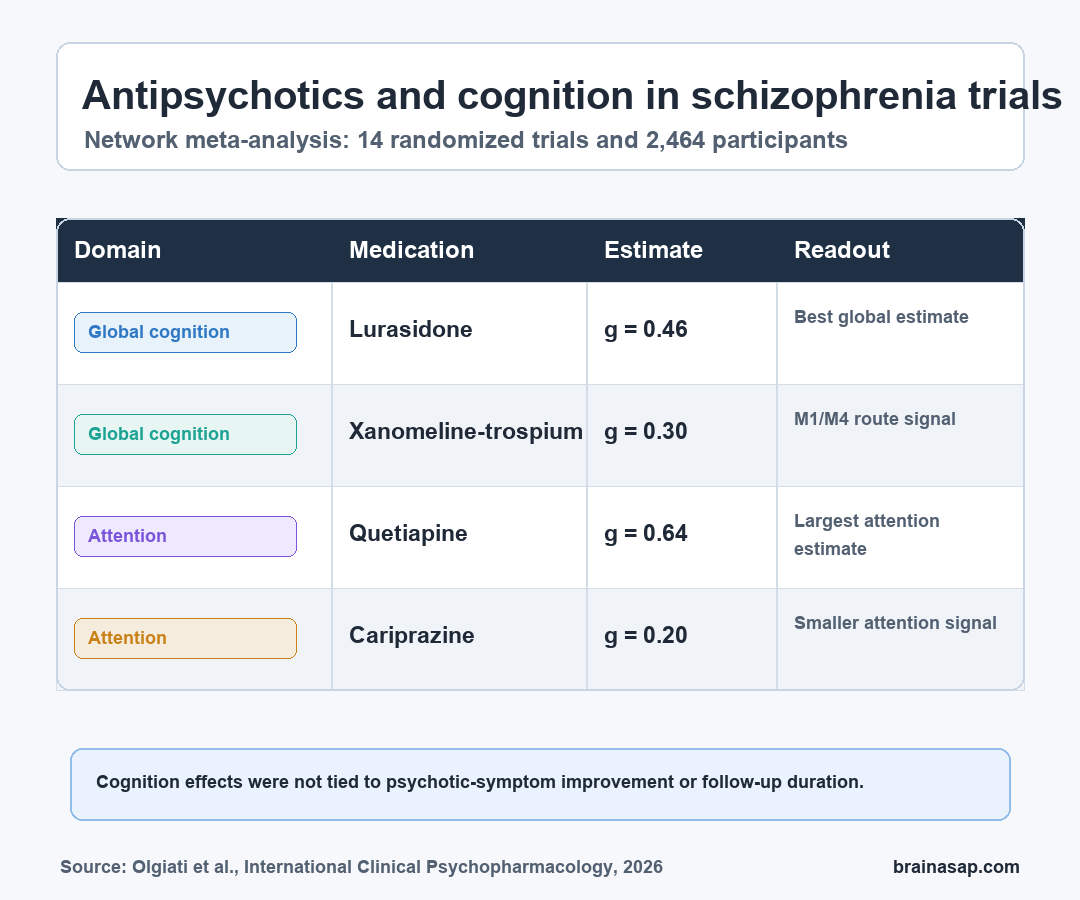
- 14 randomized trials: Researchers analyzed 2,464 participants across trials of selected second- and third-generation antipsychotics plus xanomeline-trospium.
- Lurasidone improved global cognition: Lurasidone outperformed placebo on global cognitive performance with Hedges’ g = 0.46.
- Xanomeline also beat placebo: Xanomeline-trospium showed a smaller but positive global cognition effect, with Hedges’ g = 0.30.
- Attention ranked differently: Quetiapine had the largest attention estimate, Hedges’ g = 0.64, followed by cariprazine at Hedges’ g = 0.20.
- Symptom change did not explain cognition: Cognitive effect sizes were not tied to follow-up duration or improvement in psychotic symptoms.
Source: International Clinical Psychopharmacology (2026) | Olgiati et al.
Cognitive dysfunction in schizophrenia is often treated as a background problem, but it is one of the main reasons patients struggle with work, social function, planning, memory, and daily independence.
Antipsychotics are usually judged by hallucinations, delusions, relapse prevention, and side effects. This review asked a narrower question: which antipsychotic strategies have randomized evidence for improving cognitive test scores?
The medication ranking differed by cognitive domain. In this analysis, lurasidone and xanomeline-trospium stood out for global cognitive performance, while attention outcomes favored different medications.
Network Meta-Analysis Compared Cognitive Effects Across Antipsychotic Trials
Researchers reviewed randomized controlled trials in schizophrenia-spectrum disorders and combined newly eligible studies with earlier trial evidence for antipsychotics that had potential procognitive effects.
The final network meta-analysis included 14 randomized controlled trials and 2,464 participants.
Researchers compared changes in cognitive test performance using standardized mean differences, which let them place different cognitive scales on a common effect-size metric.
The medication set covered several treatment classes:
- Third-generation antipsychotics: Cariprazine, brexpiprazole, lumateperone, and lurasidone were part of the target review question.
- Muscarinic receptor treatment: Xanomeline-trospium was included because it acts through M1/M4 muscarinic receptors rather than through the usual dopamine-first antipsychotic pathway.
- Selected second-generation comparators: Aripiprazole, olanzapine, quetiapine, risperidone, and ziprasidone were added from earlier meta-analytic evidence.
Lurasidone and Xanomeline-Trospium Led Global Cognition Results
For global cognitive performance, lurasidone outperformed placebo with Hedges’ g = 0.46. Xanomeline-trospium also outperformed placebo, with Hedges’ g = 0.30.
Those effect sizes do not mean every patient would notice a dramatic day-to-day improvement. They mean that, across randomized trial data, treated groups improved more on cognitive performance measures than placebo groups on a standardized scale.
The xanomeline-trospium result matters because muscarinic M1/M4 receptor agonism is not the classic dopamine D2 blockade route.
If replicated, the xanomeline-trospium result could widen the medication logic for cognitive symptoms in schizophrenia-spectrum disorders, especially for patients whose main disability is not fully captured by psychosis scales.
Attention Outcomes Favored Quetiapine and Cariprazine
The attention findings had a different ranking. Quetiapine had the largest favorable attention estimate, Hedges’ g = 0.64, while cariprazine followed with Hedges’ g = 0.20.
Domain-specific ranking matters because cognition is not a single symptom. Working memory, processing speed, attention, verbal learning, and executive function can move differently.
A drug that helps one domain may not be the best candidate for another. A schizophrenia trial that measures only a broad composite score could miss a useful attention effect, while an attention-heavy trial could overstate global cognitive benefit.
The paper’s practical implication is a profile-based approach:
- Global cognition problem: Lurasidone and xanomeline-trospium had the clearest placebo-separated estimates in the global outcome.
- Attention-focused problem: Quetiapine and cariprazine ranked best on attention measures in this network.
- Medication choice: Cognitive findings still have to be weighed against psychosis control, metabolic risk, sedation, movement symptoms, and patient history.
Cognitive Gains Were Not Just Psychosis Improvement
Researchers checked whether cognitive effect sizes were simply tracking the same changes as psychotic symptoms. Cognitive standardized mean differences were unrelated to follow-up duration or improvements in psychotic symptoms.
Metaregression also did not show that age or baseline psychosis severity explained the cognitive response. That does not prove the drugs directly improved cognition in every case, but it weakens the simplest explanation that cognitive gains were only a byproduct of reduced psychosis.
For clinicians and trial designers, the separation between symptom improvement and cognitive change is important. A cognitive endpoint may need its own trial design, baseline cognitive profile, and outcome hierarchy instead of being treated as an add-on to symptom-rating scales.
The paper also supports a practical reporting standard. Schizophrenia medication trials should state whether a cognitive result is global, domain-specific, or exploratory, because those labels change how the result should be used in treatment planning.
The Evidence Is Useful, But Still Not Personalized Enough
The review gives a structured map of current randomized evidence, but it does not solve medication selection for an individual patient. Network meta-analyses combine trials that can differ in sample, dose, duration, cognitive battery, illness stage, and comparator design.
The main interpretation should stay bounded:
- Promising evidence: Selected antipsychotics and xanomeline-trospium showed measurable cognitive advantages over placebo in specific domains.
- Not a full treatment algorithm: The estimates do not tell clinicians to switch a stable patient automatically based on cognition alone.
- Next research need: Future trials should match medication mechanisms to baseline cognitive profiles and functional outcomes.
The strongest takeaway is that cognition deserves direct measurement in schizophrenia-spectrum treatment research. If cognitive impairment is one of the main drivers of disability, then medication trials should treat cognitive outcomes as central endpoints, not secondary afterthoughts.
Citation: DOI: 10.1097/yic.0000000000000607. Olgiati et al. Impact of selected second and third generation antipsychotics on cognitive dysfunction in schizophrenia-spectrum disorders. Systematic review and network meta-analysis. International Clinical Psychopharmacology. 2026.
Study Design: Systematic review and frequentist network meta-analysis of randomized controlled trials.
Sample Size: 14 randomized controlled trials with 2,464 participants.
Key Statistic: Lurasidone improved global cognition versus placebo with Hedges’ g = 0.46; xanomeline-trospium improved global cognition with Hedges’ g = 0.30.
Caveat: Trial differences in dose, cognitive testing, follow-up, and participant profiles limit patient-level medication selection.