TL;DR: A 2026 study in Journal of Medical Case Reports described organophosphate-induced delayed neuropathy (OPIDN), a delayed nerve-injury syndrome, in a 44-year-old pesticide applicator after years of low-level exposure without a typical acute poisoning crisis.
Key Findings
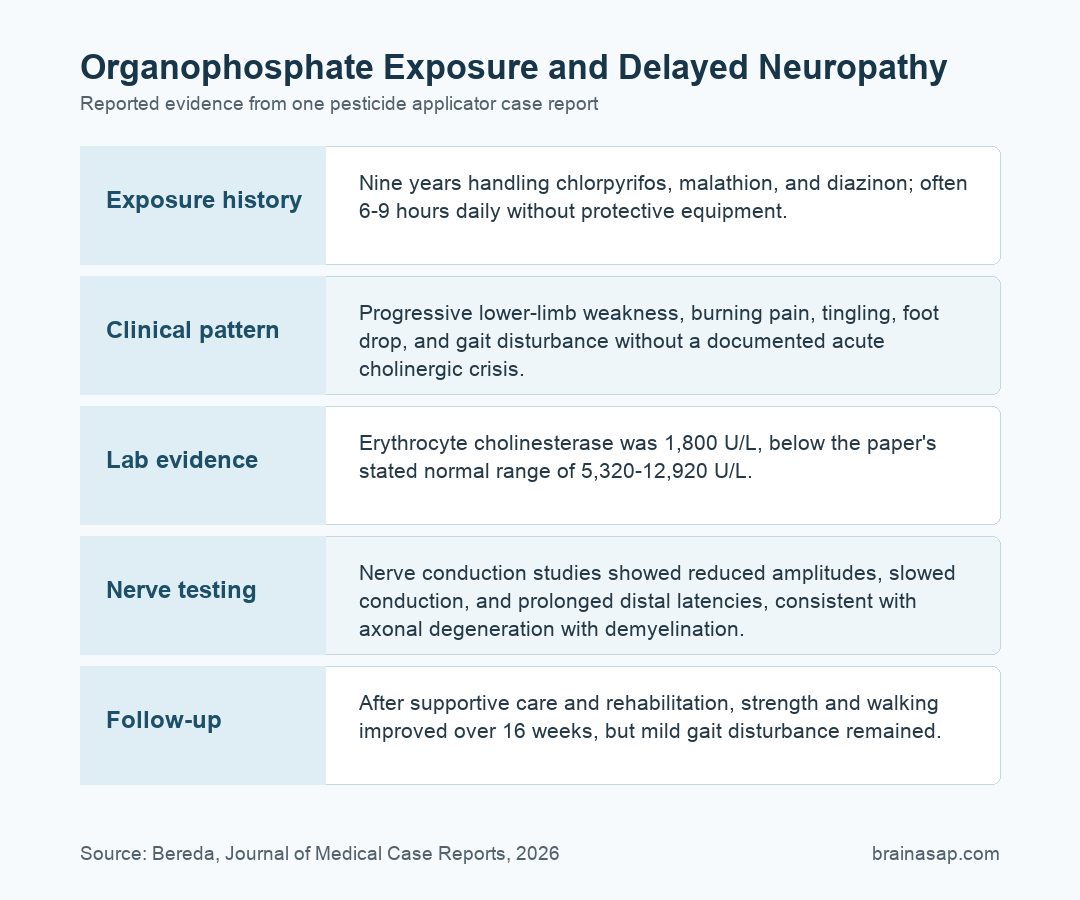
- 9-year exposure history: The patient had worked with chlorpyrifos, malathion, and diazinon for years, often 6-9 hours daily without personal protective equipment.
- No cholinergic crisis: Caregiver history did not report classic acute organophosphate poisoning symptoms such as salivation, vomiting, diarrhea, or muscle twitching.
- Marked cholinesterase reduction: Serum erythrocyte cholinesterase was 1,800 U/L, well below the paper’s stated normal range of 5,320-12,920 U/L.
- Nerve testing supported injury: Nerve conduction studies showed reduced amplitudes, slowed conduction, and prolonged distal latencies consistent with axonal degeneration with demyelination.
- Partial recovery over 16 weeks: After supportive care and rehabilitation, strength, spasticity, pain, and walking function improved, but mild gait disturbance persisted.
Source: Journal of Medical Case Reports (2026) | Bereda
Long-Term Pesticide Work Preceded Delayed Neuropathy
Organophosphates are pesticide chemicals that can interfere with nervous-system signaling. Acute poisoning is usually recognized because it causes a cholinergic syndrome: sweating, salivation, diarrhea, vomiting, muscle twitching, breathing problems, or altered consciousness soon after exposure.
This case report focused on a different pattern. A 44-year-old male pesticide applicator developed progressive lower-limb weakness, burning pain, tingling, balance problems, and difficulty walking after long-term occupational exposure rather than a single documented poisoning event.
The source history named three organophosphate pesticides: chlorpyrifos, malathion, and diazinon. The patient reportedly handled them for years in poorly ventilated agricultural settings and often without gloves, masks, or other protective equipment.
- Years 1-5: Headache, dizziness, mild fatigue, and tingling or numbness appeared intermittently.
- Years 6-8: Muscle cramps, tremor, grip difficulty, leg weakness, and leg pain became more prominent.
- Year 9: Progressive weakness, gait disturbance, nighttime burning pain, and mild memory or concentration problems were reported.
Nerve Conduction Tests Supported Mixed Nerve Injury
By hospital presentation, the neurological pattern was not just subjective pain. Examination showed bilateral lower-limb weakness, calf atrophy, absent lower-limb reflexes, distal sensory loss, foot drop, and an unsteady gait requiring assistance.
Researchers reported reduced compound muscle action potential (CMAP) amplitudes, slowed conduction velocities, and prolonged distal latencies. CMAP is the electrical response recorded from muscle after a motor nerve is stimulated; smaller amplitudes can reflect loss of functioning motor nerve fibers.
Sensory nerve action potentials (SNAPs), the sensory-nerve equivalent of that signal, were also abnormal. Together, the findings pointed toward axonal degeneration with demyelination, meaning both the nerve fiber and its insulating myelin layer appeared affected.
The case also included a markedly reduced cholinesterase value. Cholinesterase is an enzyme family that organophosphates inhibit; the reported 1,800 U/L erythrocyte cholinesterase result supported toxic exposure even though the history lacked a classic acute crisis.
OPIDN Can Appear After the Initial Exposure Window
Organophosphate-induced delayed neuropathy is usually discussed as a delayed complication after acute poisoning. Symptoms often emerge days to weeks later, commonly with distal weakness, sensory changes, cramping pain, foot drop, and gait impairment.
This case report argued that chronic, low-level occupational exposure can also fit the syndrome. Workers may not connect gradual neurologic symptoms to pesticide handling when there was no dramatic poisoning event.
- Exposure history: The patient had repeated occupational contact with organophosphates for about 9 years.
- Neurological pattern: Weakness, sensory loss, foot drop, and gait disturbance fit delayed neuropathy better than a purely metabolic or hereditary explanation.
- Testing pattern: Nerve conduction findings supported a peripheral nerve process rather than an isolated complaint of pain or fatigue.
- Exclusion workup: The report stated that fasting glucose, thyroid function, vitamin B12, folate, liver, and kidney tests were not explanatory.
The paper discussed neuropathy target esterase (NTE), a nervous-system enzyme linked to OPIDN, as one possible biological route. The proposed mechanism is not a direct proof in this single patient, but it gives the clinical pattern a plausible toxic-neurology framework.
Recovery Followed Supportive Care, Not a Proven Cure
Treatment in the report was mainly supportive. The patient received oxygen for low oxygen saturation, gabapentin for neuropathic pain, baclofen for spasticity, vitamin C and vitamin E supplementation, physical therapy, gait rehabilitation, and an ankle-foot orthosis.
The care team also gave intravenous methylprednisolone, a steroid, off label. The report framed this as a possible anti-inflammatory approach, but it is not established standard therapy for OPIDN and cannot be credited as the reason the patient improved.
- Pain control: Neuropathic pain improved from a reported visual analog score of 7 at baseline to 3 by week 16.
- Motor function: Proximal and distal lower-limb strength improved from roughly 2/5 to 4/5 over follow-up.
- Spasticity: Clinician-rated spasticity improved from moderate-to-severe values toward milder scores.
- Function: Walking improved, but residual weakness and mild gait disturbance remained.
The cleanest clinical lesson is not that one medication reversed the neuropathy. Occupational history, nerve testing, symptom management, and sustained rehabilitation can identify and manage delayed organophosphate neurotoxicity.
The Case Has Important Documentation Limits
This is a single-patient case report, so it cannot estimate how often long-term pesticide exposure causes OPIDN or how much exposure is required. It also cannot separate the effect of rehabilitation from medications, supplements, steroid treatment, or natural recovery.
Some documentation details require caution. The report described severe impairment of consciousness and low oxygen saturation alongside a delayed peripheral neuropathy picture, and repeat EMG or cholinesterase testing was not available because of financial constraints.
- Best-supported claim: The case links a long occupational exposure history with a delayed neuropathy pattern and abnormal cholinesterase and nerve conduction findings.
- Weaker claim: The case does not prove that methylprednisolone or antioxidant supplementation changed the recovery course.
- Practical implication: Chronic pesticide workers with progressive gait, sensory, or weakness symptoms need occupational exposure history taken seriously.
The clinical takeaway is concrete: delayed neurotoxicity can be missed when clinicians only look for an acute poisoning episode. Slow-onset weakness, burning pain, foot drop, and sensory loss can still belong in the organophosphate exposure differential.
Citation: DOI: 10.1186/s13256-026-06019-6. Bereda G. Long-term organophosphate exposure leading to delayed neuropathy in a pesticide applicator: a case report. Journal of Medical Case Reports. 2026.
Study Design: Single-patient occupational neurotoxicity case report.
Sample Size: 1 male pesticide applicator, age 44.
Key Statistic: Erythrocyte cholinesterase was 1,800 U/L versus the paper’s stated normal range of 5,320-12,920 U/L.
Caveat: A case report can identify a plausible clinical pattern but cannot prove treatment efficacy or population-level risk.





