TL;DR: A 2026 cross-sectional study in PLOS One found that people with post COVID-19 condition reported worse quality of life, fatigue, sleep, psychological wellbeing, and subjective cognition than COVID-19 survivors without the condition, while many objective lung, metabolic, and cognitive tests did not differ.
Key Findings
- 139-person Dutch cohort: The study included 87 people with self-reported post COVID-19 condition and 52 without it.
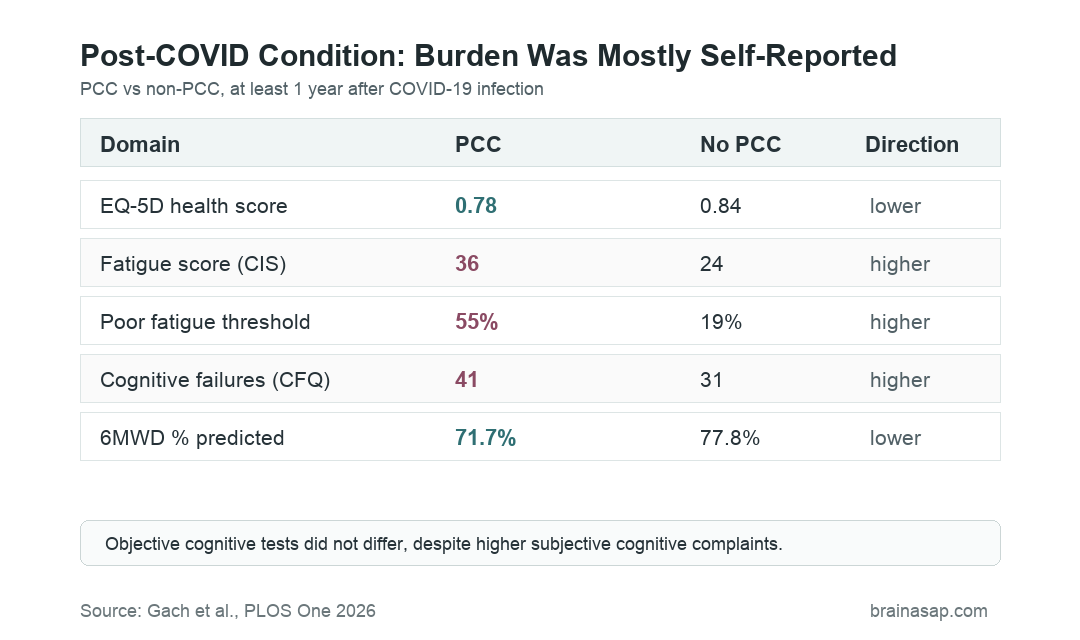
- Lower quality of life: EQ-5D scores were 0.78 in the PCC group versus 0.84 without PCC, and visual analogue health scores were 70 versus 80.
- More severe fatigue: Checklist Individual Strength fatigue scores were 36 in the PCC group versus 24 without PCC; 55% versus 19% crossed the severe-fatigue threshold.
- More subjective cognitive problems: Cognitive Failure Questionnaire scores were 41 with PCC versus 31 without PCC, but Montreal Cognitive Assessment (MoCA) scores did not differ.
- Limited objective differences: Inspiratory muscle strength and 6-minute walking distance percent predicted were lower with PCC, while pulmonary function, metabolic health, and objective cognitive tests were similar.
Post COVID-19 condition (PCC) is usually defined by persistent symptoms after SARS-CoV-2 infection that are not explained by another diagnosis. Fatigue, concentration problems, sleep disruption, dyspnea, anxiety, and depression can all appear in the clinical picture.
The Dutch COVID CLIMATE Consortium study asked a practical question: do people who report PCC also show broad objective abnormalities across lung function, metabolism, muscle strength, physical capability, and cognition?
Post-COVID Condition Was Linked to Lower Quality of Life
The study included 139 participants from three hospitals in the Netherlands. All had previously had COVID-19, and the multidimensional assessment occurred after at least one year of follow-up.
The PCC group included 87 participants; the comparison group included 52 participants without self-reported PCC. Mean age in the PCC group was 59 years, and 68% were male.
Quality-of-life differences were clear. The EQ-5D health index was lower in the PCC group: 0.78 versus 0.84. The EQ-5D visual analogue score was also lower: 70 versus 80.
Impairment rates showed the same direction:
- EQ-5D impairment: 63% with PCC versus 37% without PCC.
- VAS impairment: 47% with PCC versus 17% without PCC.
- Usual activities problems: 59% with PCC versus 27% without PCC.
- Mobility problems: 38% with PCC versus 15% without PCC.
Fatigue, Sleep, Depression, Stress, and Loneliness Were Higher
Symptoms and wellbeing measures separated the groups more clearly than many objective tests. The PCC group had higher fatigue and poorer sleep scores.
On the Checklist Individual Strength fatigue scale, scores averaged 36 with PCC versus 24 without PCC. Severe fatigue was reported by 55% of the PCC group compared with 19% of the non-PCC group.
Sleep quality also differed. Pittsburgh Sleep Quality Index scores averaged 7 with PCC versus 5 without PCC.
The psychological and social measures pointed in the same direction:
- Anxiety/depression: Hospital Anxiety and Depression Scale scores were higher in the PCC group.
- Depression threshold: Abnormal depression scores appeared in 21% with PCC versus 4% without PCC.
- Stress: Perceived Stress Scale scores were higher with PCC.
- Loneliness: Loneliness Scale scores were higher with PCC.
Subjective Cognitive Problems Increased, but MoCA Scores Did Not
The cognitive result is clinically important because many people with PCC describe “brain fog” or daily cognitive difficulty. This study measured both subjective and objective cognition.
The subjective measure was the Cognitive Failure Questionnaire (CFQ). Scores averaged 41 in the PCC group versus 31 without PCC, and 36% with PCC crossed the abnormal CFQ threshold compared with 14% without PCC.
The objective screen was the Montreal Cognitive Assessment (MoCA), a brief cognitive screening test. Mean MoCA scores and the proportion of impaired MoCA scores were similar between groups.
The gap should not be used to dismiss the cognitive complaints. The researchers noted that MoCA may miss subtle or fluctuating deficits in attention, executive function, or cognitive fatigability.
Fatigue, sleep disruption, stress, and mood symptoms may also shape how people experience daily cognitive failures.
Lung and Metabolic Tests Mostly Did Not Separate PCC
The objective testing told a narrower story. Pulmonary function, residual CT abnormalities, body composition, cardiometabolic risk, expiratory muscle strength, limb strength, mobility scores, physical activity level, and objective cognitive testing were not different between groups.
Two physical measures did differ. Maximal inspiratory pressure was lower with PCC, at 91.1% predicted versus 102.9% predicted. Six-minute walking distance percent predicted was also lower: 71.7% versus 77.8%.
The absolute 6-minute walking distance was 476 meters with PCC versus 500 meters without PCC, but that difference was not statistically significant. Both groups also averaged below 80% predicted, so functional limitation was not confined to the PCC group.
- No lung-function split: FEV1, FVC, DLCO, TLC, and residual CT abnormalities were comparable.
- No metabolic split: Body composition and cardiometabolic risk markers did not differ.
- No activity split: Step counts and activity scores were comparable.
- Partial physical signal: Inspiratory strength and 6-minute walk percent predicted were lower with PCC.
Patient-Reported Burden Should Not Be Dismissed
The study’s strongest message is a mismatch. People with PCC reported more fatigue, poor sleep, depression, stress, loneliness, and cognitive failures, but standard objective tests captured only part of that burden.
That mismatch has a practical implication. A normal lung test, metabolic panel, or brief cognitive screen does not necessarily mean the patient’s day-to-day health burden is absent.
The main limitations are also important. PCC status was based on self-report, the study was cross-sectional, most participants were recruited through hospital-linked cohorts, and the groups differed at baseline in hospitalization, smoking history, and comorbidity.
The result supports a multidimensional assessment strategy: combine objective measures with patient-reported symptoms, sleep, mood, social wellbeing, and daily cognitive function. For long COVID care, the measurable burden may sit as much in lived function as in standard clinical tests.
Citation: DOI: 10.1371/journal.pone.0352332. Gach et al. Long-term multidimensional health status of individuals with and without post COVID-19 condition: A cross-sectional study. PLOS One. 2026;21:e0352332.
Study Design: Cross-sectional multidimensional health assessment of COVID-19 survivors with and without self-reported post COVID-19 condition.
Sample Size: 139 participants, including 87 with PCC and 52 without PCC.
Key Statistic: Severe fatigue was reported by 55% with PCC versus 19% without PCC, while objective MoCA cognitive screening did not differ between groups.
Caveat: PCC was self-reported, and the cross-sectional design cannot determine why subjective burden and objective test results diverged.