TL;DR: A 2026 narrative review in Neurological Research and Practice argued that Parkinson’s prevention is most actionable through physical activity, Mediterranean-style diet patterns, toxin reduction, earlier prodromal detection, and better rehabilitation after diagnosis.
Key Findings
- Fastest-growing neurological disorder: The review described Parkinson’s disease as the fastest-growing neurological disorder worldwide.
- 6.2 to 11.8 million cases: A cited analysis found the number of people living with Parkinson’s nearly doubled within 5 years.
- Exercise risk reduction: Moderate-to-vigorous physical activity was associated with Parkinson’s risk reductions of up to 60% in epidemiological studies.
- Lifestyle and toxin targets: Mediterranean or MIND diet patterns and caffeine or tea intake were listed as protective factors, while pesticides and trichloroethylene were listed as risk factors.
- Rehabilitation evidence is stronger after diagnosis: Multidisciplinary rehabilitation and moderate-to-high intensity exercise had the broadest evidence base for tertiary prevention.
Source: Neurological Research and Practice (2026) | Schaeffer et al.
Parkinson’s disease prevention sounds simple until the stage of prevention is named. Preventing a first diagnosis, delaying conversion in a prodromal person, and preventing complications after diagnosis are different clinical problems.
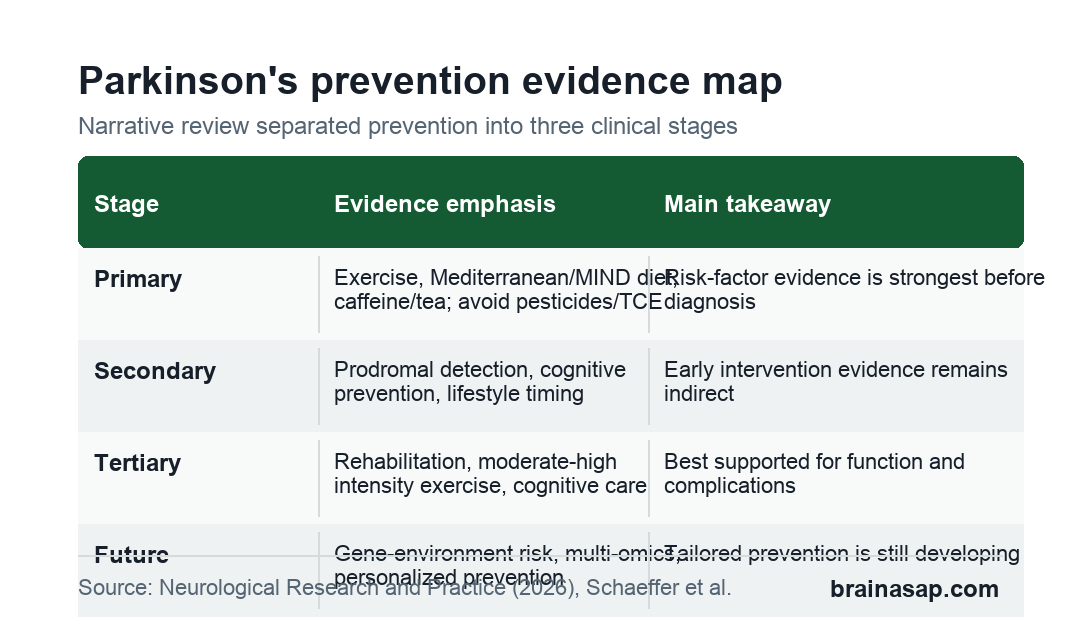
The review authors organized the field around those 3 stages. The review focused mainly on Parkinson’s disease because it has the largest movement-disorder prevention literature and the largest public-health challenge.
Parkinson’s Prevention Starts Before a Diagnosis
The review framed primary prevention around modifiable risk and protective factors. Age and genetics still matter, but lifestyle and environmental exposures are the areas where prevention research can become practical.
The best-supported primary prevention factors included:
- Physical activity: Higher activity, especially moderate-to-vigorous exercise, was associated with lower Parkinson’s risk in epidemiological studies.
- Diet patterns: Mediterranean and MIND diet adherence were listed as protective lifestyle factors.
- Caffeine or tea intake: Coffee, caffeine, or tea consumption appeared in the review’s protective-factor summary.
- Toxin reduction: Pesticides, solvents such as trichloroethylene, air pollution, and ultra-processed food were listed as risk-side exposures.
The exercise finding is the most concrete single number in the review. Epidemiological studies reported Parkinson’s risk reductions of up to 60% for moderate-to-vigorous exercise.
The authors also cautioned that some low activity in midlife could reflect early, subtle motor changes rather than a causal risk factor. That is why exercise evidence is promising but not equivalent to a randomized prevention trial.
Prodromal Parkinson’s Raises a Harder Prevention Question
Secondary prevention means identifying people before classical Parkinson’s motor diagnosis and intervening early enough to slow progression. Isolated rapid eye movement sleep behavior disorder, genetic risk, smell loss, constipation, and other prodromal markers can help define higher-risk groups.
The review was careful about the evidence here. Early detection has improved, but systematic therapeutic intervention in the prodromal phase remains limited.
For lifestyle factors, the support is mostly indirect:
- Exercise timing: Moderate physical activity has been associated with later disease onset, but this does not prove prodromal disease modification.
- Diet timing: Mediterranean or MIND diet adherence has also been associated with later onset in some studies.
- Ultra-processed food: Higher ultra-processed food consumption has been associated with earlier onset, which needs more direct testing.
The ethical issue is important. Telling someone they may be in a prodromal Parkinson’s phase carries psychological weight when no proven disease-modifying drug is available.
Education about exercise, diet, sleep, and toxin reduction can give patients some agency, but clinicians still need to avoid implying that lifestyle change can guarantee prevention.
Pesticides, TCE, Air Pollution, and Ultra-Processed Food Were Risk Targets
The review did not frame prevention only as personal lifestyle. Environmental exposures were part of the risk map, especially pesticides, solvents such as trichloroethylene (TCE), air pollution, and ultra-processed food.
Public health prevention needs more than clinic counseling. Exercise counseling can be done in a clinic, but pesticide exposure, solvent regulation, food environment, and air quality require workplace, agricultural, regulatory, and community-level action.
The authors also listed traumatic brain injury and type 2 diabetes as relevant risk-side factors. Those items connect Parkinson’s prevention to injury prevention, metabolic health, and broader chronic-disease policy rather than a single neurology clinic visit.
Rehabilitation Has the Strongest Post-Diagnosis Evidence
Tertiary prevention starts after Parkinson’s disease is diagnosed. The goal is to prevent complications, preserve daily function, and maintain quality of life.
This area has a broader evidence base than prodromal intervention. The review highlighted physiotherapy, occupational therapy, speech therapy, cognitive training, and multidisciplinary rehabilitation models.
Exercise remains central after diagnosis:
- Moderate-to-high intensity training: The review described strong evidence for this approach, even though it is not consistently translated into routine practice.
- Multidisciplinary care: Coordinated rehabilitation can address movement, swallowing, speech, cognition, and daily functioning.
- Cognitive impairment: Early diagnosis and treatment of cognitive impairment are recommended but remain insufficiently integrated into routine care.
The gap is not only scientific. It is also operational: reimbursement, access, clinician training, and long-term adherence determine whether rehabilitation evidence becomes normal care.
Personalized Parkinson’s Prevention Is Still Developing
The review pointed toward personalized prevention as a long-term goal. Parkinson’s risk is shaped by gene-environment interactions, environmental toxins, prodromal markers, lifestyle, comorbidities, and possibly multi-omics profiles.
A future prevention plan may combine polygenic risk, exposure history, sleep behavior, smell testing, movement markers, microbiome data, and blood or imaging biomarkers. For now, most of that remains research infrastructure rather than everyday clinical care.
The current practical message is more modest and more usable. Encourage physical activity, support Mediterranean-style dietary patterns, reduce avoidable toxin exposure, identify prodromal risk carefully, and treat rehabilitation as prevention after diagnosis.
Those steps do not replace disease-modifying therapy. They define the prevention work that can move forward while pharmacological disease modification remains unavailable.
Citation: DOI: 10.1186/s42466-026-00488-2. Schaeffer et al. Preventing Parkinson’s disease in the context of movement disorders: a narrative review of current evidence and future directions. Neurological Research and Practice. 2026;8:27.
Study Design: Narrative review prioritizing systematic reviews, meta-analyses, randomized trials, and large prospective cohort studies.
Sample/Model: Parkinson’s disease prevention literature across primary, secondary, and tertiary prevention stages.
Key Statistic: Epidemiological studies reported Parkinson’s risk reductions of up to 60% for moderate-to-vigorous exercise.
Caveat: Primary and secondary prevention evidence remains largely observational or indirect; causal prevention trials are still limited.