TL;DR: A 2026 review in Journal of Pain Research argues that postoperative pain care is moving away from opioid-centered prescribing toward multimodal, opioid-sparing protocols, with the strongest practical signal around NSAIDs paired with dexamethasone or regional anesthesia and the largest unresolved gap after hospital discharge.
Key Findings
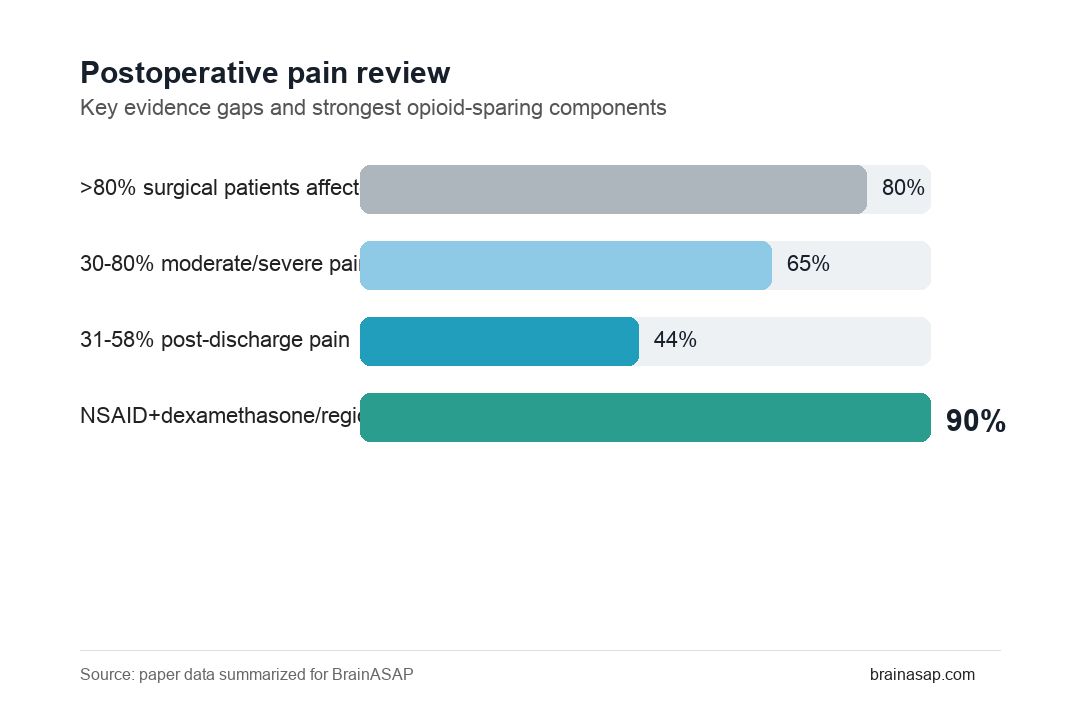
- More than 80% affected: The review describes postoperative pain as a common clinical problem affecting more than 80% of surgical patients, with moderate-to-severe pain reported in roughly 30% to 80% depending on procedure and definition.
- 31% to 58% after discharge: Pain can persist beyond hospitalization in 31% to 58% of patients, where monitoring is thinner and opioid stewardship is less standardized.
- NSAID combinations stood out: Current evidence identified NSAIDs combined with dexamethasone or regional anesthesia as among the most clinically meaningful opioid-sparing strategies.
- Precision tools remain early: Pharmacogenomics, machine-learning pain prediction, biosignal monitoring, and wearables are promising but not yet routine perioperative standards.
- Post-discharge protocols lag behind ERAS: Enhanced Recovery After Surgery programs have strengthened inpatient multimodal care, but outpatient dosing, education, tapering, and follow-up remain inconsistent.
Source: Journal of Pain Research (2026) | Sezerano and Niyonkuru
Postoperative pain management is not just a question of whether a patient receives enough analgesia in the recovery room. The review frames it as a perioperative-to-home problem: pain intensity, functional recovery, opioid exposure, patient education, and follow-up all interact after surgery.
Opioid-centered care can reduce pain but also increases risks of nausea, sedation, constipation, falls, tolerance, opioid-induced hyperalgesia, persistent use, and leftover tablets in the community.
Opioid-Centered Postoperative Pain Care Leaves a Discharge Gap
The review starts from a practical mismatch. Hospitals increasingly use Enhanced Recovery After Surgery (ERAS) protocols, but many patients leave with variable instructions and opioid prescriptions that may exceed actual need.
Sezerano and Niyonkuru describe several linked problems:
- High pain burden: Moderate-to-severe pain remains common even when standard analgesics are used.
- Variable prescribing: Discharge opioid quantities often reflect clinician habit more than patient-level risk.
- Limited monitoring: Once patients leave the hospital, pain, adverse effects, and functional recovery are harder to track.
- Persistent use risk: Poorly managed acute pain and excess opioid exposure can contribute to chronic postsurgical pain or prolonged opioid use.
The review does not argue that opioids have no place. Its point is narrower: opioids should be one component of a planned analgesic strategy, not the organizing center of postoperative care.
NSAIDs, Dexamethasone, and Regional Anesthesia Had the Clearest Opioid-Sparing Role
The paper reviews pharmacologic options including acetaminophen, NSAIDs, gabapentinoids, ketamine, dexmedetomidine, intravenous lidocaine, tramadol, opioids, and glucocorticoids.
Across that broad landscape, the clearest practical distinction is between components with consistent opioid-sparing value and components whose role is narrower or more procedure-specific.
- NSAIDs and COX-2 inhibitors: Useful non-opioid analgesics when kidney, bleeding, gastrointestinal, and cardiovascular risks are acceptable.
- Dexamethasone: A perioperative glucocorticoid with analgesic and antiemetic roles, often discussed as an adjunct to reduce pain and nausea.
- Regional anesthesia: Nerve blocks and neuraxial techniques can reduce systemic opioid exposure but require expertise and can cause rebound pain or motor impairment.
- Acetaminophen: Common and generally safe at appropriate dosing, but the review suggests its incremental opioid-sparing contribution may be smaller than often assumed.
Multimodal Analgesia Works Best When the Combination Is Procedure-Specific
Multimodal analgesia means combining drugs and techniques that act through different mechanisms. The goal is not to add every possible agent; it is to reduce pain while avoiding avoidable toxicity.
The review repeatedly cautions that good multimodal care depends on patient and procedure context:
- Procedure type: A nerve block that helps one orthopedic operation may not fit another surgery.
- Patient risk: Older adults, kidney disease, anticoagulation, respiratory disease, and psychiatric vulnerability can change the safety profile.
- Recovery goal: Analgesia should support walking, breathing, sleep, rehabilitation, and discharge readiness, not only lower a pain score.
- Medication interaction: NSAIDs, SSRIs, anticoagulants, sedatives, opioids, and gabapentinoids can interact in clinically important ways.
That is why the review favors standardized but flexible protocols. A good protocol narrows variation while still allowing clinicians to adjust for risk.
Machine Learning, Pharmacogenomics, and Wearables Are Promising but Not Settled
The authors also review newer precision tools. Pharmacogenomic-guided prescribing could help identify patients who metabolize opioids or adjunctive drugs unusually, especially through pathways such as CYP2D6.
Machine-learning models may help predict pain intensity, opioid need, or high-risk recovery patterns by combining clinical variables, biosignals, and procedure details. Some biosignal-based postoperative pain models have reported accuracy above 80% in small cohorts, but that does not make them ready for unsupervised clinical decisions.
- Potential benefit: Earlier identification of high-risk patients could guide closer follow-up and safer discharge plans.
- Implementation barrier: Models need external validation, calibration across hospitals, and workflow integration.
- Data burden: Wearables can add continuous information but also create privacy, interoperability, and alert-fatigue problems.
Post-Discharge Multimodal Pain Care Needs Stronger Trials
The largest practical gap is the least glamorous one: what happens after the patient leaves. The review argues that many ERAS gains remain hospital-centered, while post-discharge multimodal analgesia is less standardized.
Three needs come through clearly:
- Procedure-specific outpatient protocols: Discharge plans should define non-opioid schedules, opioid rescue use, tapering, and red flags.
- Long-term outcomes: Trials should measure chronic postsurgical pain, function, opioid persistence, and return to normal activity.
- High-risk subgroup evidence: Older adults, adolescents, chronic-pain patients, opioid-exposed patients, and patients with psychiatric comorbidity need dedicated data.
The review separates a mature idea from an unfinished system. Multimodal, opioid-sparing pain care is no longer experimental, but the exact combinations, outpatient protocols, and precision tools still need stronger evidence.
Citation: DOI: 10.2147/JPR.S597049. Sezerano ML, Niyonkuru E. Personalized multimodal and opioid-sparing analgesia for postoperative pain management: enhancing recovery and addressing the post-discharge gap. Journal of Pain Research. 2026;19:597049.
Study Design: Narrative review of multimodal and opioid-sparing postoperative pain strategies, including pharmacologic, regional, non-pharmacologic, digital, and precision-medicine approaches.
Sample/Model: Literature-based synthesis rather than a new patient cohort; the review cites perioperative trials, systematic reviews, implementation studies, and digital pain-monitoring work.
Key Statistic: The review identifies NSAIDs combined with dexamethasone or regional anesthesia as having the strongest opioid-sparing role, while highlighting persistent post-discharge protocol gaps.
Caveat: This is a review, not a new randomized trial; conclusions depend on heterogeneous studies, variable surgery types, and inconsistent long-term outcome reporting.