TL;DR: A 2026 BJPsych Bulletin paper argues that person-first language in forensic mental health services may reduce stigma, social distance, and pessimism when it is used carefully rather than as a substitute for structural change.
Key Findings
- Forensic mental health focus: The editorial examines labels used for people receiving care at the intersection of psychiatry and criminal justice.
- Consistent stigma pattern: Prior studies linked person-first terms to lower blame, lower social distance, and more rehabilitative attitudes.
- Large media experiment: In a nationally representative US sample of 2,800 people, criminal labels produced more negative associations than person-first wording.
- Forensic sample evidence: A UK randomised study of 668 people found lower desired social distance for recovery-oriented person-first language.
- Cautious implementation: The authors recommend practical language changes while acknowledging limits, identity preferences, and structural coercion.
Source: BJPsych Bulletin (2026) | Tomlin, Mitisheva, Kilbane, Markham, and Tully
Forensic care records can move through ward notes, tribunals, family conversations, academic papers, and news coverage. A label that starts as shorthand can become the frame through which a person is judged.
The Tomlin editorial focuses on a setting where people may be called patients, service users, offenders, prisoners, mentally disordered offenders, or diagnoses such as schizophrenic and psychotic.
The authors’ point is not that wording alone repairs stigma. Their argument is narrower: labels can shape how others assign blame, danger, treatability, and social distance, so forensic mental health services should choose words with more precision.
Forensic Mental Health Labels Can Add Criminal Justice Stigma to Illness Stigma
Forensic mental health services sit between healthcare and the criminal justice system. Labels are therefore especially loaded.
A person can be described by a diagnosis, a legal status, past behaviour, service status, or risk assessment all at once.
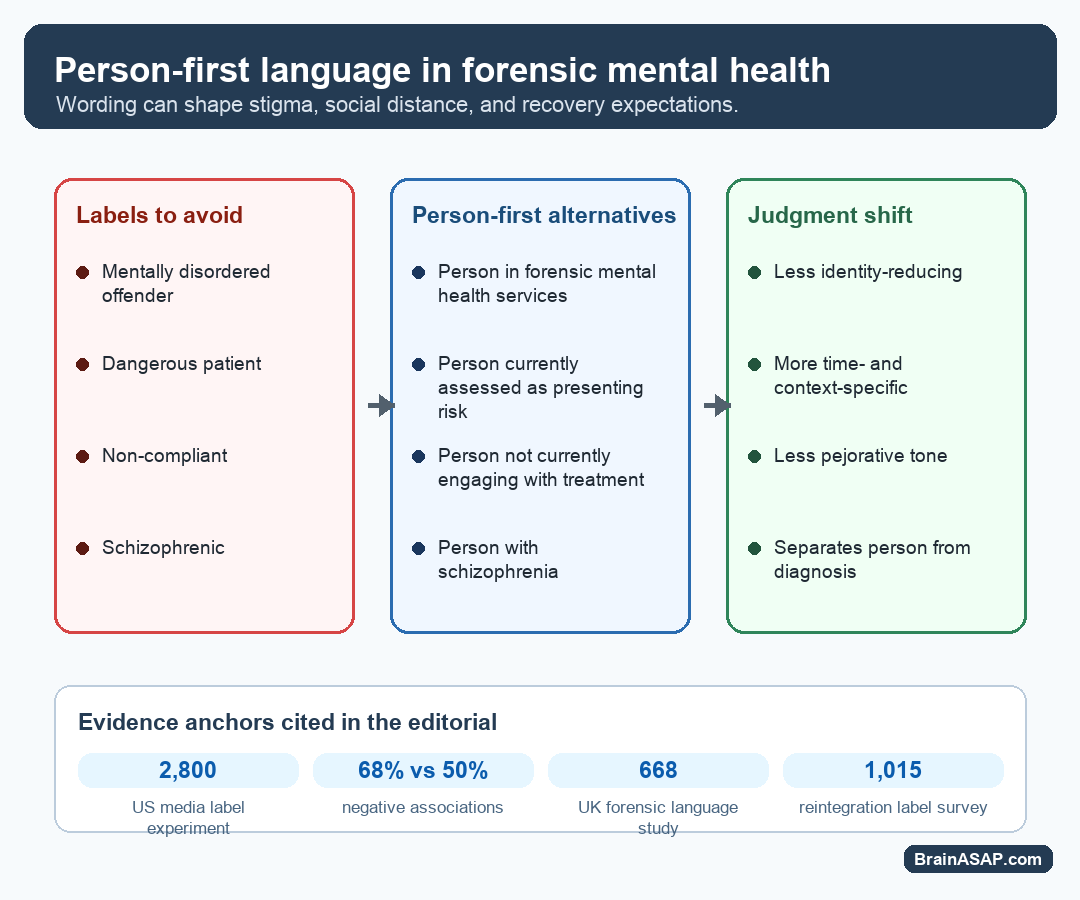
The editorial contrasts identity-reducing labels with phrases that keep the person in view. For example, “mentally disordered offender” can be replaced by “person in forensic mental health services” when legal precision does not require the older phrase.
- Clinical identity: Patient, service user, client, or person receiving support can frame the interaction as care.
- Legal identity: Detained, sectioned, restricted, or under a hospital order can frame the person by compulsion.
- Risk identity: Dangerous, resistant, or non-compliant can turn a temporary behaviour into a fixed trait.
- Diagnostic identity: Schizophrenic or psychotic can collapse a person into a diagnosis.
The person-first alternative is not always shorter. Its value is that it can be more exact.
“Person currently assessed as presenting risk” says something different from “dangerous patient”, because it leaves room for context, time, and reassessment.
Person-First Language Was Linked to Less Blame and Social Distance
The editorial summarizes evidence from substance use, mental illness, criminal justice, and forensic mental health studies. Much of the evidence comes from surveys and experiments that test how people respond to different labels.
Two substance-use studies found that “people with substance use disorders” produced less blame and less punitive judgment than “substance abusers”.
A US study of 701 students and counselling trainees found that “people with mental illness” was linked to less authoritarian and socially restrictive attitudes than “the mentally ill”.
- 2,800-person media experiment: Person-first criminal justice wording, such as “person with a felony conviction,” produced fewer negative associations than labels such as “felon.”
- 68% versus 50%: Negative associations were chosen by 68% of participants in the criminal-label condition versus 50% in the person-first condition.
- 668-person forensic study: “Person working towards recovery using forensic mental health services” lowered desired social distance compared with “forensic mental health patient” or “mentally disordered offender.”
- 1,015-person reintegration study: “Person who was formerly incarcerated” was linked to lower stereotypes and lower desired social distance than “ex-convict.”
These results do not prove that every person-first phrase will work in every setting. They do show a repeated pattern: when labels foreground a stigmatized category, observers often respond with more distance and more negative assumptions.
Forensic Psychiatry Language May Shape Treatability and Recovery Expectations
The editorial describes several mechanisms that could explain why wording is important. One is power.
Labels applied by institutions can reinforce the idea that the labelled person is inferior or permanently outside the community.
A second mechanism is essentialism, the tendency to treat a label as part of a person’s underlying nature.
If someone is described mainly as an offender, schizophrenic, or dangerous patient, the label can seem fixed rather than situational.
- Internalized stigma: Repeated labels can shape how a person sees themselves.
- Treatment avoidance: People may avoid services when identifying language is shaming or dehumanizing.
- Prognostic pessimism: Fixed labels can make improvement seem less likely.
- Rehabilitation attitudes: Recovery-oriented terms can make care, agency, and change easier to imagine.
This is especially important in forensic care because the goal is not only symptom management. Services also work with safety, rehabilitation, autonomy, and reintegration.
Language that keeps a person separate from a legal route into care may support more reflective clinical thinking.
Practical Changes Include Notes, Codes of Practice, Teaching, and Media Style
The editorial gives concrete examples rather than asking services to adopt a vague politeness rule. It suggests changes in mental health legislation, codes of practice, clinical notes, academic writing, education, and media reporting.
For example, “restricted patient” or “sectioned patient” can become “person receiving support under the Mental Health Act” when that wording is accurate.
“Non-compliant” can become “person not currently engaging with treatment”, which describes the observed behaviour without turning it into character.
- Clinical notes: Use behaviour-specific wording, especially for engagement, mistrust, and risk.
- Legal documents: Preserve legal meaning while avoiding unnecessary identity labels.
- Academic writing: Model neutral terms such as “person in forensic mental health services.”
- Media reporting: Avoid diagnosis-as-identity labels unless a community preference or direct context supports them.
Useful person-first language is not euphemism. It should make the description more accurate, less fatalistic, and less likely to blur diagnosis, risk, legal status, and personhood.
Person-First Language Has Limits in Forensic Mental Health Practice
The editorial is careful about what language can and cannot do. Changing terms does not remove coercion, poverty, racism, service underfunding, trauma, or public fear.
It also does not guarantee that a new term will stay free of stigma.
Some groups prefer identity-first language because it can support shared identity and community. Affected groups may reject person-first language in some contexts.
Forensic mental health also involves victims, public safety, involuntary treatment, and serious harms, so language should not be used to hide those realities.
- What the editorial supports: Cautious adoption of person-first language where it improves precision, dignity, and recovery orientation.
- What it does not settle: Whether every service user, family, victim, clinician, or community will prefer the same terms.
- What still needs study: Real-world effects on clinical interactions, stigma, service engagement, staff attitudes, and unintended consequences.
- Best practical test: Use language that is accurate enough for care and respectful enough to avoid turning a status into an identity.
The practical conclusion is modest: forensic mental health language should describe what is clinically or legally relevant without making a person sound reducible to illness, offending, detention, or risk.
Citation: DOI: 10.1192/bjb.2026.10230. Tomlin et al. The value of person-first language in forensic mental health services. BJPsych Bulletin. 2026:1-4.
Study Design: Editorial and evidence synthesis on person-first language in forensic mental health services.
Sample Size: No new participant sample; the editorial cites prior survey and experimental studies, including samples of 2,800, 701, 668, and 1,015 people.
Key Statistic: In a 2,800-person US media experiment cited by the authors, criminal-label wording produced negative associations in 68% of participants versus 50% with person-first wording.
Caveat: The editorial supports cautious implementation, but it does not test a new clinical intervention or prove that wording changes alone reduce real-world coercion, discrimination, or risk outcomes.