TL;DR: A 2026 study in Molecular Psychiatry found that radiofrequency capsulotomy and inferior thalamic peduncle deep brain stimulation were associated with the largest symptom improvements among surgical strategies for refractory obsessive-compulsive disorder.
Key Findings
- 75 studies: The network meta-analysis included 75 studies, 1,259 patients, and 20 surgical strategies for refractory obsessive-compulsive disorder.
- Y-BOCS was primary: The main outcome was change in Yale-Brown Obsessive Compulsive Scale (Y-BOCS), a clinician-rated OCD symptom-severity scale.
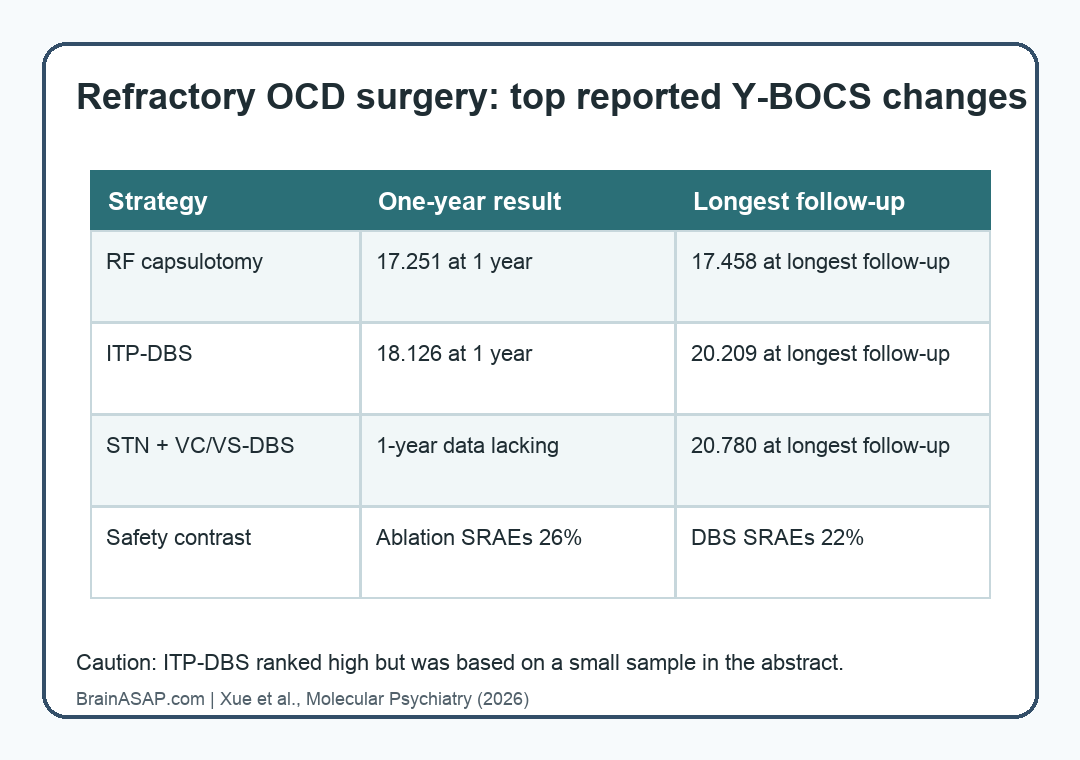
- RF capsulotomy led at 1 year: Radiofrequency capsulotomy was associated with a 17.251-point Y-BOCS improvement at 1 year and 17.458 points at longest follow-up.
- ITP-DBS also ranked high: Inferior thalamic peduncle deep brain stimulation was associated with 18.126-point improvement at 1 year and 20.209 points at longest follow-up.
- Ablation had more surgical adverse events: Ablative surgery had a higher surgery-related adverse-event rate than DBS, 26% versus 22%, while serious adverse events did not differ significantly.
Source: Molecular Psychiatry (2026) | Xue et al.
Refractory OCD Surgery Compared Ablation and DBS Targets
Refractory obsessive-compulsive disorder (OCD) refers to severe OCD that has not responded adequately to standard treatments. In the surgical literature, two broad strategies dominate: lesion-based procedures and adjustable stimulation.
Ablative surgery creates a targeted lesion in a circuit thought to drive symptoms. Deep brain stimulation (DBS) implants electrodes and adjusts electrical stimulation over time.
Both approaches are reserved for highly selected patients because they are invasive. Candidates usually have severe symptoms despite medication, exposure-based psychotherapy, and specialist psychiatric care.
The researchers used a network meta-analysis, which lets analysts compare several treatments even when many have not been tested head-to-head. Their source pool covered 20 surgical strategies across 75 studies.
- Ablative procedures: Capsulotomy, cingulotomy, limbic leucotomy, and related lesion approaches.
- DBS approaches: Targets including inferior thalamic peduncle, subthalamic nucleus, ventral capsule/ventral striatum, and combined targets.
- Main scale: Y-BOCS, where lower scores mean fewer OCD symptoms.
Radiofrequency Capsulotomy and ITP-DBS Had the Largest Improvements
Most surgical strategies were associated with significant Y-BOCS improvement. The typical reduction was around 10 to 15 points, but several approaches ranked higher.
Radiofrequency capsulotomy (RF-Cap) was among the strongest performers. The mean difference was 17.251 points at 1 year and 17.458 points at longest follow-up.
Inferior thalamic peduncle DBS (ITP-DBS) also ranked near the top, with a 18.126-point improvement at 1 year and 20.209 points at longest follow-up. The authors caution that the ITP-DBS evidence came from a smaller sample, so that ranking should be interpreted carefully.
Y-BOCS point changes are clinically important because the scale is built around obsessions, compulsions, distress, resistance, control, and functional interference. A 10-point reduction can be meaningful in severe illness, so the reported top-ranked effects are large enough to matter if they hold up in direct comparisons.
Combined STN Plus VC/VS DBS Looked Strong at Longest Follow-Up
Another high-ranking result came from subthalamic nucleus plus ventral capsule/ventral striatum DBS, abbreviated STN plus VC/VS-DBS. At longest follow-up, this combined target had a mean Y-BOCS improvement of 20.780 points.
The limitation is timing. The abstract reports that 1-year data were lacking for this combined DBS strategy, so its comparison with RF-Cap and ITP-DBS is not as complete.
The timing distinction changes the clinical interpretation. A strong longest-follow-up result may reflect durable benefit, selection effects, uneven follow-up, or differences in who received a given procedure.
Network meta-analysis can organize the evidence, but it cannot replace direct randomized comparisons among targets.
Ablation Had More Surgery-Related Adverse Events Than DBS
The safety results separated ordinary surgery-related adverse events from serious adverse events. Ablative surgery had a higher surgery-related adverse-event rate than DBS: 26% versus 22%, with p = 0.0325.
The highest surgery-related adverse-event rate was reported for mechanical capsulotomy, at 47.5%. Serious adverse events did not differ significantly between DBS and ablative surgery.
The safety distinction is especially relevant because ablation and DBS ask patients to accept different tradeoffs. DBS has implanted hardware, battery management, programming visits, and device-related risks.
Ablation avoids device maintenance but leaves a permanent lesion.
- DBS advantage: Stimulation can be adjusted, reduced, or stopped, though the implanted system carries hardware and programming burdens.
- Ablation advantage: Lesion procedures do not require long-term device programming, but the lesion itself is not adjustable.
- Shared concern: Both approaches are invasive and require careful psychiatric, neurosurgical, and ethical selection.
The Evidence Still Needs Head-to-Head Surgical Trials
The analysis supports surgical intervention as a serious option for a narrow group of patients with refractory OCD. It does not imply that surgery belongs anywhere near first-line treatment.
The authors’ own conclusion is cautious: RF-Cap and ITP-DBS had the largest improvements, but ITP-DBS relied on a small sample, and more head-to-head studies are needed.
The available file also has a practical limitation. It was a captured primary article page and abstract rather than the complete Springer full-text PDF, so this summary sticks to the reported abstract-level outcomes.
- Best-supported headline: RF-Cap and ITP-DBS ranked highest for Y-BOCS improvement.
- Most important safety split: Ablation had more surgery-related adverse events than DBS.
- Main uncertainty: Surgical targets still need direct comparative studies in carefully defined refractory OCD populations.
The right interpretation is not that one operation is the universal best OCD surgery. The more defensible point is that surgical OCD evidence is becoming target-specific, and the strongest candidates need direct comparison.
Citation: DOI: 10.1038/s41380-025-03438-7. Xue et al. Comparative efficacy and safety of different surgical strategies for refractory obsessive-compulsive disorder: evidence from network meta-analysis. Molecular Psychiatry. 2026;31:2978-2989.
Study Design: Network meta-analysis of surgical strategies for refractory OCD.
Sample Size: 75 studies involving 1,259 patients and 20 surgical strategies.
Key Statistic: ITP-DBS was associated with a 20.209-point Y-BOCS improvement at longest follow-up, while RF-Cap showed 17.458 points.
Caveat: The ITP-DBS estimate came from a small sample, and the available file provided abstract-level results rather than a full-text PDF.