TL;DR: A 2026 study in Implementation Science Communications found that high-performing HEALing Communities Study coalitions used representative membership, shared goals, data support, and communications campaigns to strengthen opioid-use-disorder service implementation.
Key Findings
- 8 communities studied: Researchers selected the top-performing urban and rural waitlist-control communities from each of four HEALing Communities Study sites.
- 41 interviews analyzed: Coalition-member interviews were conducted at the end of the implementation phase and analyzed thematically.
- OUD services stayed difficult: High-performing communities still faced persistent barriers to opioid-use-disorder service delivery and access.
- Coalition structure mattered: Representative membership, high engagement, shared goals, and collaboration supported implementation success.
- No urban-rural theme split: The analysis reported no major theme differences between selected urban and rural communities.
Source: Implementation Science Communications (2026) | Walker et al.
Opioid-use-disorder (OUD) programs often depend on community coalitions, not only clinics. The question in this qualitative study was why some local coalitions were better able to implement evidence-based overdose prevention and treatment practices.
The study focused on top performers in the HEALing Communities Study, a large effort built around the Communities That HEAL approach.
HEALing Communities Study Coalitions Were Selected for High Implementation Performance
The HEALing Communities Study tested ways to increase use of overdose education and naloxone distribution (OEND) and medication for opioid use disorder (MOUD). Both are evidence-based practices for reducing opioid overdose harm.
Researchers used a positive-deviance design: instead of comparing average communities, they selected high-performing waitlist-control communities for deeper study. The top urban and rural community from each of the four HCS sites was chosen.
- Case count: The analysis included 8 high-performing communities.
- Interview count: Researchers analyzed 41 coalition-member interviews.
- Framework: Coding was aligned with the PRISM/RE-AIM implementation framework.
That design makes the study less about whether coalitions work in general and more about what supported strong implementation in communities that were already doing relatively well.
The interview sample also shows who supplied the qualitative evidence. Among the 41 interviewees, 24 represented urban communities and 17 represented rural communities.
Most participants identified as female, non-Hispanic, and White, and more than half had at least a bachelor’s degree.
Those details matter for interpretation because coalition-member interviews capture the view from implementation partners. They do not directly capture every patient, family, clinician, or community resident affected by OUD services.
High-Performing OUD Coalitions Still Faced Service Barriers
Top performance did not mean easy implementation. Interviewees still described persistent and varied barriers related to OUD service delivery and access.
The finding needs a systems-level reading because OEND and MOUD implementation depends on local conditions. Community stigma, treatment access, service coordination, policy shifts, and existing health infrastructure can all shape whether evidence-based practices reach people who need them.
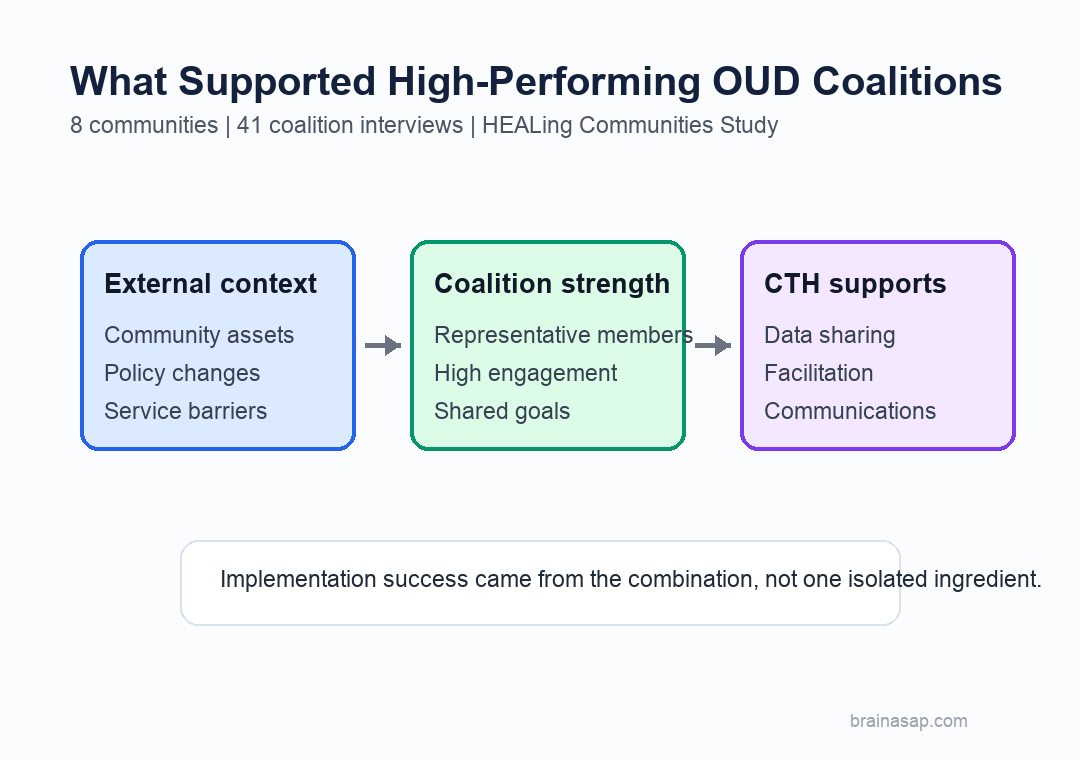
The study also found that community assets and policy changes provided a foundation for improvement. Strong coalitions were responding to real local constraints and opportunities, not implementing a generic playbook.
Representative Membership and Shared Goals Supported OUD Implementation
The clearest internal-coalition theme was representative membership. High-performing coalitions included people who understood different parts of the local OUD response, rather than relying on one sector alone.
High engagement and alignment with coalition goals also mattered. Participants described collaboration and a shared vision for the community, which helped maintain buy-in to the implementation process.
- Representation: Coalitions benefited from members who reflected relevant community systems and service roles.
- Engagement: Active participation helped communities move from planning to implementation.
- Shared direction: Common goals made it easier to select and sustain strategies.
For OUD work, that structure is practical. Naloxone distribution, medication treatment, and communications campaigns usually cross healthcare, behavioral health, public health, criminal-legal, and community organizations.
The coalition findings also clarify why membership alone is not enough. A large coalition can still struggle if members are not engaged, do not share goals, or cannot translate local data into feasible actions.
Data Sharing and Communications Campaigns Helped Coalitions Choose Strategies
The Communities That HEAL process also contributed to implementation success. Coalition buy-in to the process helped communities use facilitation, data-driven decision-making, and communications work rather than treating them as outside requirements.
Structured data connectivity and sharing helped coalitions choose strategies more effectively. Multi-channel communications campaigns were reported to increase awareness and uptake of OUD and MOUD services.
- Data support: Local information helped coalitions identify feasible and impactful strategy targets.
- Communications: Campaigns increased awareness, acceptance, and service uptake.
- Coalition buy-in: Members were more likely to use the CTH process when it fit local goals.
The study did not report major theme differences across urban and rural communities. The selected communities still had local differences, but the cross-cutting implementation themes were similar in the high-performing sites.
That urban-rural result is narrow. It applies to the eight selected higher-performing communities, not to every rural or urban OUD coalition.
Positive-Deviance Design Limits the Opioid Coalition Claims
The study deliberately examined higher-performing communities. That design identifies factors linked with stronger implementation, but it does not show whether the same themes were absent in lower-performing communities.
The interview sample also limits generalization. Participants were mostly female, non-Hispanic White, highly educated coalition members, so their views may not represent every community member affected by OUD services.
The most practical reading is a concrete checklist for implementation teams: build representative coalitions, keep goals shared, connect data to decisions, and use communications campaigns to make OUD and MOUD services visible.
Citation: DOI: 10.1186/s43058-026-00952-9. Walker et al. The role of external and internal context on adoption and implementation of evidence-based practices: a serial case study qualitative analysis of top performers in the HEALing Communities Study. Implementation Science Communications. 2026.
Study Design: Positive-deviance nested serial case study with thematic analysis of coalition-member interviews.
Sample Size: 8 high-performing communities and 41 coalition-member interviews.
Key Statistic: The top urban and rural community from each of four HEALing Communities Study sites was selected for in-depth case study.
Caveat: The study focused on higher-performing communities and did not test whether the same themes differed in lower-performing communities.